As a rule of thumb, the more you pay attention to Canada’s political circus, the worse your state of mental health becomes, IMO anyway. On a more serious note, David Clinton got curious about a recent Manhattan Institute project tracing American mental health trends:

Image from The Audit
The Manhattan Institute’s research into the confluence of mental health trends and political leanings in the U.S. generated buzz a while back. Among other things, they discovered that, as of the 2021-22 school year, liberal students were 13-17 percent more likely to seek mental health treatment than their conservative peers. That’s a frightening gap.
I was curious to know if there’s anything like that going on here in Canada. And it turns out that there’s excellent public-facing data waiting for us to drop by and help ourselves. The most recent published version of the Canadian Election Study (CES) dates back to the period around the 2021 federal election — the full dataset from 2025 isn’t yet available.
There were 20,968 respondents in total in the CES survey data from 2021. Having now spent a couple of happy hours with the results, this looks like an excellent representation of Canadian society. The questions go both deep and wide.1
I was able to directly address the political angle to all this using responses to one core question. Participants were asked to situate themselves on a political “scale where 0 means the left and 10 means the right”.
I classified anyone who responded with a number higher than 6 as “far right”, and responses less than 4 were tagged “far left”. The far left cohort had 4,927 members, while there were just 3,891 people in the far right. Those numbers are easily large enough to make distinctions potentially statistically meaningful.
Anxiety
I explored both far right and far left cohorts for how accurately the words “anxious” and “easily upset” applied to them. A response of seven indicates a self-assessment of extreme anxiety, while zero would be Big-Lebowski-level calm.
The average for the right-coded group was 3.47, while those on the left rated themselves 3.88.
Overall Mental Health
Respondents were asked to rate their mental health in relation to their peers where “1” indicates excellent mental health and “5” indicates poor mental health. A total of 3,878 from the far right responded and 3,263 from the far left. The average of all responses on the right was 2.02 (standard deviation: 0.876859) and from the left, 2.32 (0.926268).
- In fact, the average survey took two hours and twenty five minutes to complete! I’m definitely glad they didn’t ask me.
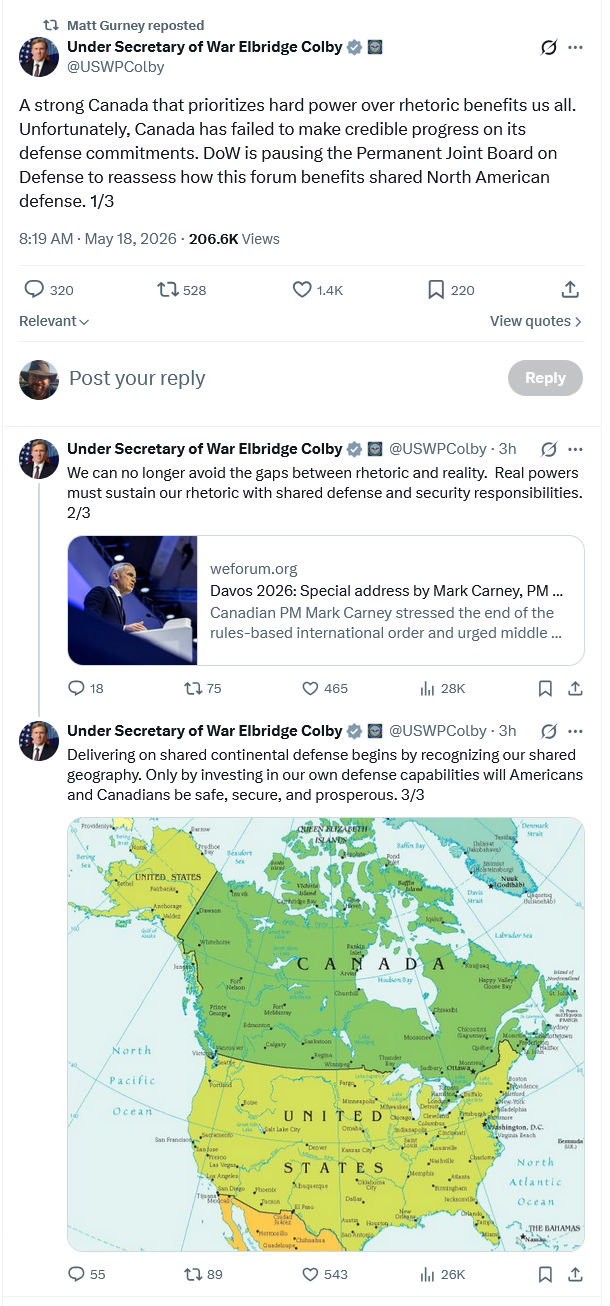
I mentioned the other day that the US was fully justified in “pausing” their participation in the Permanent Joint Board on Defence due to the Canadian government’s continued delinquence on military matters (and Prime Minister Carney’s blatant desire to tweak American noses while neglecting joint interests with the United States. At The Line, Matt Gurney says this won’t be the only tangible sign of American impatience with our ongoing fecklessness:
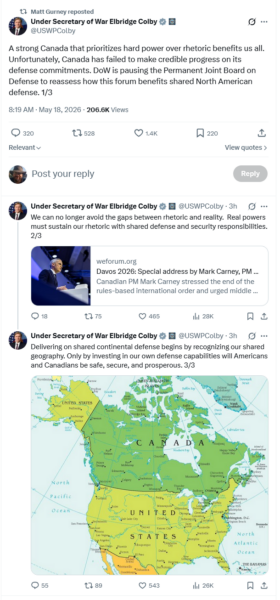
As I posted on social media when sharing this: “This is another gentle reminder to the f*ckwits in the Canadian government that they are playing with existential fire when they work to actively piss off our American allies.”
First of all, and this will annoy the Elbows Uppers to no end, the undersecretary’s comments are, fundamentally, accurate. Canada has indeed massively underinvested in defence and has also prioritized rhetoric over reality. I completely understand why Canadians hate admitting this — I hate admitting this. Having your flaws pointed out to you by someone you dislike is always a mortifying experience. But I’ve spent almost two decades writing about the very things Colby is pointing out — Canada has allowed its military capability to atrophy to a point, as I noted just a week ago in an episode of On The Line, where we’ll need many years and untold billions of dollars just to rehabilitate the armed forces. Expanding them and adding capabilities will be a whole other level of investment. This is why Canada’s recent major announcements on defence, though good and welcome, are also not enough — it will take a long time and even more money to actually repair what we have allowed to rot.
The other half of what Colby identified is also, alas, accurate. While we were massively underfunding defence and allowing core capabilities to wither and die, or while just totally missing the bus on transformational military developments (hello, drones!), Canada did indeed talk a lot about the rules-based international order and the role of middle powers and punching above our weight and all the rest. Canada focusing on rhetoric instead of reality is, alas, a fair criticism.
Many U.S. administrations called us out on this. We ignored them. Donald Trump is unique in how viciously he is prepared to exploit our weakness, but he’s hardly the first to have noticed it and called us out on it. I carry no water for MAGA or Trump, but they’ve got us dead to rights on this one. The bad orange man didn’t let the navy rust out, repeatedly defer the fighter jet replacement and hobble the army with non-serviceable equipment and recruiting and procurement systems that were actually quite awful at both those things.
We did those things. We did it to ourselves. Colby is simply possessed of the gall to bluntly call us out on our failures, in a way that Canadians aren’t accustomed to and aren’t going to enjoy.
So that’s part of it. But it’s also worth asking why the U.S. is doing this, and especially why they’re doing it now.
Part of it, probably, is just sincere frustration with us. As noted above, Colby’s remarks are accurate. But the timing is interesting. The CUSMA renegotiation deadline looms in early July And in Colby’s remarks, do I detect a whiff of the art of the deal?
The Carney government has made, and continues to make, plenty of announcements about plans, and potential deals, and future capabilities, and so on … but the Americans can’t help but notice that little is actually being done despite all the sound and fury on the PR side. Canada belatedly reached the long-agreed-upon 2% of GDP target for military spending, but most of it was a bookkeeping exercise of moving existing costs onto the Department of National Defence budget (the Canadian Coast Guard and parts of Veterans Affairs) but not much improved in Canada’s actual defence capabilities.