
You know how drug companies pay six or seven figures for thirty-second television ads just on the off chance that someone with the relevant condition might be watching? You know how they employ drug reps to flatter, cajole, and even seduce doctors who might prescribe their drug? Well, it turns out that having 15,000 psychiatrists in one building sparks a drug company feeding frenzy that makes piranhas look sedate by comparison. Every flat surface is covered in drug advertisements. And after the flat surfaces are gone, the curved sufaces, and after the curved surfaces, giant rings hanging from the ceiling.
The ads overflow from the convention itself to the city outside. For about two blocks in any direction, normal ads and billboards have been replaced with psychiatry-themed ones, until they finally peter off and segue into the usual startup advertisements around Market Street.
Scott Alexander, “The APA Meeting: A Photo-Essay”, Slate Star Codex, 2019-05-22.
July 20, 2023
QotD: Advertising to a semi-captive audience
July 6, 2023
“Too many complaints? That’s racism. Too few complaints? Well, that’s racism, too.”
Amy Eileen Hamm reports on how the British Columbia College of Nurses and Midwives (BCCNM) acted on its concern that not enough complaints against their members were being lodged by First Nations people:
As regular readers of Quillette will know, many Canadian institutions have fervently adopted the cause of “decolonization” — a vaguely defined term that one university describes as the dismantling of “assumed Euro-western disciplinary constructs and traditions”. This can mean anything from abolishing musical scales (which “perpetuate and solidify the hegemony of [the] Euro-American repertoire”); to reimagining our scientific understanding of sunlight, so as to correct “the reproduction of colonialism” that has infected “physics and higher physics education”; to assailing the gender binary through a “decolonizing act of resistance”.
That’s the theory, anyway. In practice, institutional efforts at “decolonization” generally translate into affirmative-action hiring programs and policies to mandate symbolic (generally empty) gestures such as land acknowledgements. They’ve also created a cash cow for “specialist” administrators and third-party consultants in what is now known as the “equity, diversity, inclusion, and decolonization” sector. The premise is that decolonization is so difficult and complex that it can only be overseen by said (highly paid) professionals.
My own professional sector, nursing, provides a useful case study. In British Columbia, where I live and work, nurses are licenced by the British Columbia College of Nurses & Midwives (BCCNM), whose offices are located “on unceded Coast Salish territory, represented today by the Musquea?m, Squamish and Tsleil-Waututh Nations.” In other words, Vancouver.
If a patient feels that he or she has experienced “incompetent, unethical, or impaired nursing or midwifery practice”, he or she can complain to the BCCNM through its complaints portal. It’s not a complicated process. You send an email describing what the nurse allegedly did, when the incident occurred, and whether there were any witnesses. If you’ve already complained to someone else, you’re supposed to note that as well, along with your suggestions for resolving the complaint. That’s it.
But apparently, this process is just too onerous — and even dangerous — for Indigenous people. And so the BCCNM has paid C$97,000 to a self-described “boutique business process management firm” called Novatone, which has duly produced a lengthy report on how to “make the BCCNM complaints process safer for Indigenous Peoples.” The same title — mantra might be a better word — appears at the top of all 50 pages: Looking Back to Look Forward: How Indigenous ways of being, knowing, and doing must inform the BCCNM feedback process and reflect the principles of cultural safety, cultural humility, and anti-racism.
(For the benefit of those outside Canada, the mystical-sounding phrase, “ways of knowing”, along with its “being” and “doing” variants, has now entered the official idiom as a means to signify the unfalsifiable shaman-like intuitions that supposedly guide the consciousness of Indigenous people throughout every facet of their existence — including, apparently, complaining about the care they receive from nurses.)
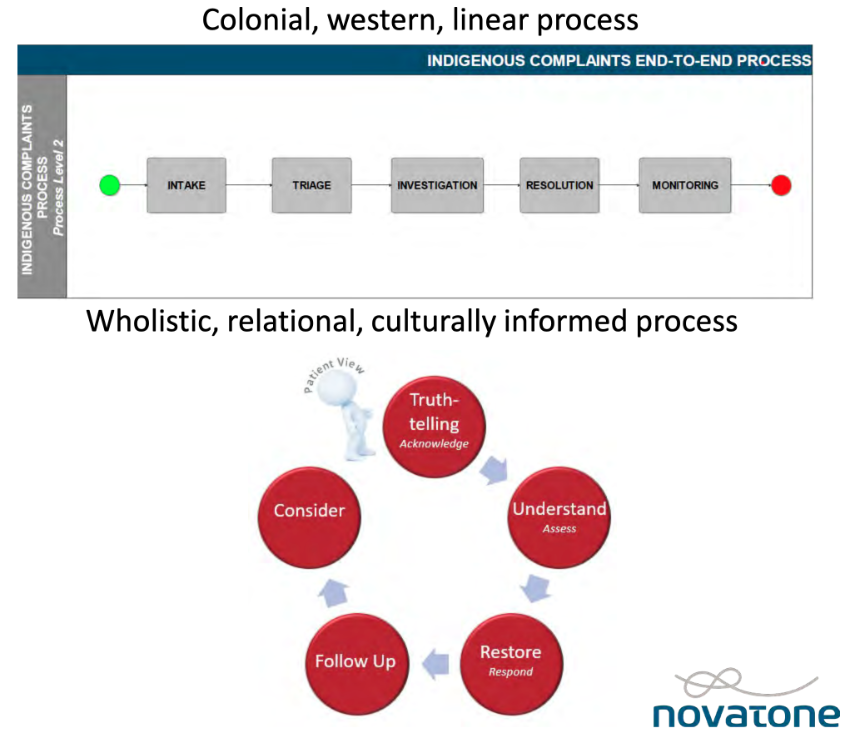
Juxtaposed images from the Novatone report, Looking Back to Look Forward, contrast the “colonial, western, linear” nature of existing BCCNM processes with a “wholistic, relational, culturally informed process” that would supposedly align with Indigenous values.
June 15, 2023
Thursday tab-clearing
A few items that I didn’t feel required a full post of their own, but might be of interest:
- Justin Trudeau’s government is clearly interested in moving to a Central Bank Digital Currency (CBDC), but “Canadians are not at peace with the idea of cash vanishing into thin air, with a consistent 80 per cent of respondents having no plans to go cashless“
- There’s an ongoing shortage of Adderall in the United States … and the Drug Enforcement Agency (DEA) is behind it.
- Alasdair Beckett-King explains what’s wrong with every time travel movie – https://youtu.be/zI0aBzA2K9s
- The man who visited Lenin’s Soviet Union and said “I have been over into the future, and it works.”
- Kim du Toit isn’t a believer in the official inflation statistics: “When the history of this era comes to be written, one of the most egregious falsehoods to be exposed will be the ‘official’ inflation rate.”
- Random meme of the day:
April 12, 2023
Institutional Review Boards … trying to balance harm vs health, allegedly
At Astral Codex Ten Scott Alexander reviews From Oversight to Overkill by Simon N. Whitley, in light of his own experience with an Institutional Review Board’s demands:
Dr. Rob Knight studies how skin bacteria jump from person to person. In one 2009 study, meant to simulate human contact, he used a Q-tip to cotton swab first one subject’s mouth (or skin), then another’s, to see how many bacteria traveled over. On the consent forms, he said risks were near zero — it was the equivalent of kissing another person’s hand.
His IRB — ie Institutional Review Board, the committee charged with keeping experiments ethical — disagreed. They worried the study would give patients AIDS. Dr. Knight tried to explain that you can’t get AIDS from skin contact. The IRB refused to listen. Finally Dr. Knight found some kind of diversity coordinator person who offered to explain that claiming you can get AIDS from skin contact is offensive. The IRB backed down, and Dr. Knight completed his study successfully.
Just kidding! The IRB demanded that he give his patients consent forms warning that they could get smallpox. Dr. Knight tried to explain that smallpox had been extinct in the wild since the 1970s, the only remaining samples in US and Russian biosecurity labs. Here there was no diversity coordinator to swoop in and save him, although after months of delay and argument he did eventually get his study approved.
Most IRB experiences aren’t this bad, right? Mine was worse. When I worked in a psych ward, we used to use a short questionnaire to screen for bipolar disorder. I suspected the questionnaire didn’t work, and wanted to record how often the questionnaire’s opinion matched that of expert doctors. This didn’t require doing anything different — it just required keeping records of what we were already doing. “Of people who the questionnaire said had bipolar, 25%/50%/whatever later got full bipolar diagnoses” — that kind of thing. But because we were recording data, it qualified as a study; because it qualified as a study, we needed to go through the IRB. After about fifty hours of training, paperwork, and back and forth arguments — including one where the IRB demanded patients sign consent forms in pen (not pencil) but the psychiatric ward would only allow patients to have pencils (not pen) — what had originally been intended as a quick record-keeping had expanded into an additional part-time job for a team of ~4 doctors. We made a tiny bit of progress over a few months before the IRB decided to re-evaluate all projects including ours and told us to change twenty-seven things, including re-litigating the pen vs. pencil issue (they also told us that our project was unusually good; most got >27 demands). Our team of four doctors considered the hundreds of hours it would take to document compliance and agreed to give up. As far as I know that hospital is still using the same bipolar questionnaire. They still don’t know if it works.
Most IRB experiences can’t be that bad, right? Maybe not, but a lot of people have horror stories. A survey of how researchers feel about IRBs did include one person who said “I hope all those at OHRP [the bureaucracy in charge of IRBs] and the ethicists die of diseases that we could have made significant progress on if we had [the research materials IRBs are banning us from using]”.
Dr. Simon Whitney, author of From Oversight To Overkill, doesn’t wish death upon IRBs. He’s a former Stanford IRB member himself, with impeccable research-ethicist credentials — MD + JD, bioethics fellowship, served on the Stanford IRB for two years. He thought he was doing good work at Stanford; he did do good work. Still, his worldview gradually started to crack:
In 1999, I moved to Houston and joined the faculty at Baylor College of Medicine, where my new colleagues were scientists. I began going to medical conferences, where people in the hallways told stories about IRBs they considered arrogant that were abusing scientists who were powerless. As I listened, I knew the defenses the IRBs themselves would offer: Scientists cannot judge their own research objectively, and there is no better second opinion than a thoughtful committee of their peers. But these rationales began to feel flimsy as I gradually discovered how often IRB review hobbles low-risk research. I saw how IRBs inflate the hazards of research in bizarre ways, and how they insist on consent processes that appear designed to help the institution dodge liability or litigation. The committees’ admirable goals, in short, have become disconnected from their actual operations. A system that began as a noble defense of the vulnerable is now an ignoble defense of the powerful.
So Oversight is a mix of attacking and defending IRBs. It attacks them insofar as it admits they do a bad job; the stricter IRB system in place since the ‘90s probably only prevents a single-digit number of deaths per decade, but causes tens of thousands more by preventing life-saving studies. It defends them insofar as it argues this isn’t the fault of the board members themselves. They’re caught up in a network of lawyers, regulators, cynical Congressmen, sensationalist reporters, and hospital administrators gone out of control. Oversight is Whitney’s attempt to demystify this network, explain how we got here, and plan our escape.
March 30, 2023
“Nothing is as permanent as a temporary government program” … except those few that make your life easier
At Astral Codex Ten, Scott Alexander reacts to the US government’s new moves to make telehealth less useful for as many people as possible:

Telemedicine is when you see a doctor (or nurse, PA, etc) over a video call. Medical regulators hate new things, so for its first decade they ensured telemedicine was hard and inconvenient.
Then came COVID-19. Suddenly important politicians were paying attention to questions about whether people could get medical care without leaving their homes. They yelled at the regulators, and the regulators grudgingly agreed to temporarily make telemedicine easy and convenient.
They say “nothing is as permanent as a temporary government program”, but this only applies to government programs that make your life worse. Government programs that make your life better are ephemeral and can disappear at any moment. So a few months ago, the medical regulators woke up, realized the pandemic was over, and started plotting ways to make telemedicine hard and inconvenient again.
The first fruit of their labor is DEA-407, which makes it hard for telemedicine doctors to prescribe controlled substances. Controlled substances are drugs like Adderall, Ritalin, Xanax, or Ambien that the government has declared to be potentially addictive. The new rules say that telemedicine doctors can no longer prescribe these (or, in some cases, can prescribe them one time in an emergency).
Why don’t I like this decision? I am a telepsychiatrist. I work with about a hundred psychiatric patients who, for one reason or another, prefer online to physical appointments:
- Some live in small towns that don’t have psychiatrists of their own
- Some have agoraphobia, chronic pain, or some other condition that makes it hard for them to go to an office.
- Some move around a lot and like to be able to see their psychiatrist whether they’re in LA or SF.
- Some live hundreds of miles away from me, but know and trust me for some reason, and would rather see me than someone closer to them.
- Some appreciate the fact that I charge lower rates than psychiatrists who have offices, because I don’t have to pay for Bay Area commercial real estate and pass those costs on to my patients.
- Some work during work hours, and like being able to see me from their office instead of taking half the day off to travel to my location.
- Some like convenience and dislike inconvenience
As a psychiatrist, a big part of my job is prescribing controlled substances. For example, most guidelines agrees that the first-line treatment for severe ADHD is stimulant medications (eg Adderall or Ritalin). And although psychiatrists hate to admit it, the first-line treatment for temporary crisis anxiety, especially when it’s so bad that the patient isn’t able to listen to your clever plans to solve it with therapy, is benzodiazepines (eg Valium or Klonopin). You can’t be a good well-rounded psychiatrist without the option to sometimes prescribe these drugs.
“Well, your patients will have to find a different psychiatrist, or transition off of them”. Nobody ever finds different psychiatrists. Some of my patients are a bad match for my style or areas of expertise, and I’ve tried very hard to find them different psychiatrists, and it never works. Maybe there are no other psychiatrists in their area. Maybe the psychiatrists in their area don’t take the right insurance, or are too far away from mass transit. Maybe the psychiatrists have six month long wait lists. Sometimes it’s just that my ADHD patients get distracted and forget they were supposed to find new psychiatrists, and I can’t hold their hand literally all the time. As for transitioning off the medications, some patients absolutely cannot function at all without them. Did I mention that if you come off of some of them too quickly, you can literally die?
March 24, 2023
From “railway spine” to “shell shock” to PTSD
At Founding Questions, Severian discusses how our understanding of what we now label “Post-Traumatic Stress Disorder” evolved from how doctors visualized bodily ailments over a century ago:
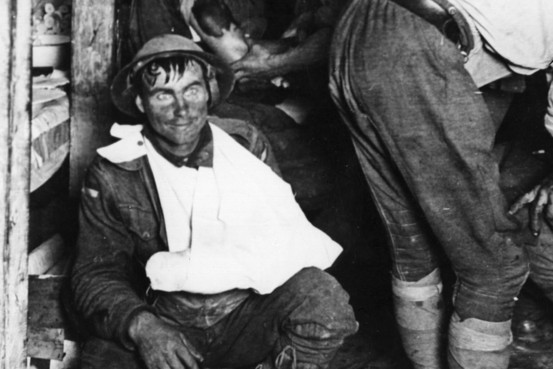
A shell-shocked and physically wounded soldier in the First World War.
I mentioned “shell shock” yesterday, so let’s start there. Medicine in 1914 was still devoted to the “Paris School,” which assumed nothing but organic etiology for all syndromes. Sort of a reverse Descartes — as Descartes (implicitly) “solved” the mind-body problem by disregarding the body, so the “Paris School” of medicine solved it by disregarding the mind. So when soldiers started coming back from the front with these bizarre illnesses, naturally doctors began searching for an organic cause. (That’s hardly unique to the Paris School, of course; I’m giving you the context to be fair to the 1914 medical establishment, whose resistance to psychological explanations otherwise seems so mulish to us).
They’d noticed something similar in the late 19th century, with industrial accidents and especially train crashes. When a train crashed, the people in the first few cars were killed outright, those in the next few wounded, but the ones in the back were often physically fine. But within a few hours to weeks, they started exhibiting all kinds of odd symptoms. Hopefully you’ve never been in a train crash, but if you’ve ever been in a fender-bender you’ve no doubt experienced a minor league version of this.I hit a deer on the highway once. Fortunately I was at highway speed, and hit it more or less dead on (it jumped out as if it were committing suicide), so it got thrown away from the car instead of coming through the windshield. The car’s front end was wrecked, naturally, but I was totally fine. I don’t think the seatbelt lock even engaged, much less the airbag, since I didn’t even have time to hit the brakes.
The next few hours to days were interesting, physiologically. It felt like my body was playing catch up. I had an “oh shit, I’m gonna crash!!!” reaction about 45 minutes after I’d pulled off to the side of the road, duct-taped the bumper back on as best I could, and continued to my destination. All the stuff I would have felt had I seen the deer coming came flooding in. Had I not already been where I was going, I would’ve needed to pull over, because that out of the blue adrenaline hit had my hands shaking, and my vision fuzzed out briefly.
The next morning I was sore. I had all kinds of weird aches, as if I’d just played a game of basketball or something. I assume part of it actually was the impact — it didn’t feel like much in the moment, but if it’s enough to crumple your car’s front end (and it was trashed), it’s enough to give you a pretty good jolt. That would explain soreness in the arms, elbows, and shoulders — a stiff-armed, white-knuckle grip on the steering wheel, followed by a big boom. But I was also just kinda sore all over, plus this generalized malaise. I felt not-quite-right for the next few days. Nothing big, no one symptom I can really put my finger on, but definitely off somehow — a little twitchy, a little jumpy, and really tired.
Having done my WWI reading, I knew what it was, and that’s when I really understood the doctors’ thought processes. I really did take some physical damage, because I really did receive a pretty good full-body whack. It just wasn’t obvious to the naked eye. And since everyone has experienced odd physical symptoms from being rattled around, or even sleeping on a couch or sprung mattress, it makes sense — the impact obviously jiggled my spine, which probably accounts for a great many of the physical symptoms. Hence, “railway spine”. And from there, “shell shock” — nothing rattles your back like standing in a trench or crouching in a dugout as thousands of pounds of high explosive go off around you. It must be like going through my car crash all day, every day.
Skip forward a few decades, and we now have a much better physiological understanding of what we now call (and I will henceforth call) Post-Traumatic Stress Disorder (PTSD). There’s a hypothesis that I personally believe, that “shell shock” is also a whole bunch of micro-concussions as well as “classic” PTSD, but let’s leave that aside for now. The modern understanding of PTSD is largely about chemistry. Cortisol and other stress chemicals really fuck you up. They have systemic physical and mental effects. If those chemicals don’t get a chance to flush out of your system — if you’re in a trench for weeks on end, let’s say — the effects are cumulative, indeed exponential.
Returning to my car crash: I was “off” for a few days because my body got a huge jolt of stress chemicals. That odd not-quite-right thing I felt was those chemicals flushing through. Had I gone to a shrink at that moment, he probably would’ve diagnosed me with PTSD. But I didn’t have PTSD. I had a perfectly normal physiological reaction to a big shot of stress chemicals. If I’d gotten into car crash after car crash, though, day in and day out, that would’ve been PTSD. I’d be having nightmares about that deer every night, instead of just the once. And all that would have cumulative, indeed exponential, effects.
He then goes on to cover similar physical reactions to stimuli in modern life, so I do recommend you RTWT.
February 16, 2023
A modern irregular verb: I mis-spoke. You spread misinformation. He has been banned from social media
I derive my headline from the original words of Bernard Woolley: “That’s one of those irregular verbs, isn’t it? I give confidential security briefings. You leak. He has been charged under section 2a of the Official Secrets Act.” It was a joke in Yes, Minister, but as Jon Miltimore shows, it’s a model for how the powers-that-be want to treat how information is shared on social media:

As Reuters reported in a recent fact-check, Mr. Gore was guilty of misrepresenting scientific data — or “spreading ‘misinformation'”.
In 2009, many responded playfully to Gore’s faux pas.
“Like most politicians, practicing and reformed, Al Gore has been known to stretch the truth on occasion”, NPR noted, adding that Gore had also claimed he’d helped create the internet.
Today, misinformation is treated in a much different way — at least in some instances. Throughout the COVID-19 pandemic, many writers and scientists who questioned the government’s use of lockdowns, mask mandates, enforced social distancing, and vaccine mandates were banned from social media platforms while others lost their jobs.
San Francisco attorney Michael Senger was permanently banned from Twitter after calling the government’s pandemic response “a giant fraud”. Prior to him, it was former New York Times reporter Alex Berenson who got the boot after questioning the efficacy of vaccines in preventing COVID-19 transmission. Months earlier it was author Naomi Wolf, a political advisor to the presidential campaigns of Bill Clinton and Al Gore.
All of these accounts were reinstated after Elon Musk purchased the company. Twitter is hardly alone, however. Facebook and YouTube also announced policies banning the spread of COVID misinformation, particularly information related to vaccines, which is what got Drs. Peter McCullough and Robert Malone ostracized and banned.
Some may argue these policies are vital, since they protect readers from false information. However, there is nothing that says Big Tech can only ban information that is false. On the contrary, in court proceedings Twitter has claimed it has “the right to ban any user any time for any reason” and can discriminate “on the basis of religion, or gender, or sexual preference, or physical disability, or mental disability”.
Facebook, meanwhile, has argued in court that the army of fact-checkers they employ to protect readers from false information are merely sharing “opinions”, and are therefore exempt from defamation claims.
[…]
What Big Tech is doing is concerning, but the fact that this censorship is taking place in coordination with the federal government makes it doubly so.
In July, in arguably the most anti-free speech pronouncement made at the White House in modern history, White House press secretary Jen Psaki noted the White House is “flagging problematic posts for Facebook”.
“We are in regular touch with these social media platforms, and those engagements typically happen through members of our senior staff, but also members of our COVID-19 team”, Psaki explained. (Today we know that these companies are staffed with dozens of former CIA and FBI officials.)
All of this is being done in the name of science, but let’s be clear: there’s nothing scientific about censorship.
February 12, 2023
QotD: The heyday of Victorian newspapers
Now, the principal quality or characteristic of the sellers of patent medicine has always been effrontery, that is to say the blatant insinuation of the false. Thomas Holloway’s innovation was to insinuate such falsehood on a mass or industrial scale. There was hardly a newspaper in which he did not place a weekly advertisement; moreover, he pioneered the advertisement that masquerades as news story. He would ensure that reports of miracle cures in faraway places, supposedly wrought by his pills and ointment, and written as matter-of-factly as possible, were placed in every newspaper, reports whose veracity no one could possibly check for himself, of course.
As Napoleon once said, repetition is the only rhetorical technique that really works — besides which hope and fear render people susceptible to effrontery. In Thomas Holloway’s time, the fear of illness was often, and the hope of cure rarely, justified; at least Holloway’s preparations were unlikely to do much harm (they contained aloe, myrrh, and saffron), unlike the prescriptions of the orthodox doctors of the time. They allowed for the possibility of natural recovery, whereas orthodox medicine often hurried its consumers into their graves. Nevertheless, the claims Holloway made for his ointment and pills were preposterous, and something is not curative just because it fails to kill.
Holloway made an immense fortune by his effrontery and founded a women’s college in the University of London on the proceeds.
Theodore Dalrymple, “The Way of Che”, Taki’s Magazine, 2017-10-28.
January 16, 2023
QotD: The avant-garde
Of course, in certain fields the latest is inclined to be best. For example, no one would wish to be treated surgically using the methods of Sir Astley Cooper: but if we want modern treatment, it is not because it is modern but because it better as gauged by pretty obvious criteria. If it were worse (as very occasionally it is), we should not want it, however modern it were.
Alas, the idea of progress has infected important spheres in which it has no proper application, particularly the arts. It is difficult to overestimate the damage that the gimcrack notion of teleology inhering in artistic endeavour has inflicted on all the arts, exemplified by the use of the term avant-garde: as if artists were, or ought to be, soldiers marching in unison to a predetermined destination. If I had the power to expunge a single expression from the vocabulary art criticism, it would be avant-garde.
Theodore Dalrymple, “Architectural Dystopia: A Book Review”, New English Review, 2018-10-04.
January 15, 2023
One last dance for Davos?
Elizabeth Nickson on the “walls closing in” but this time it isn’t “on Trump”, but it might be “on the World Economic Forum” and their enablers:
Klaus and his gang were in full egomaniacal flight last week in Davos. I wonder how secretly scared they were, swanning around in their $30,000 Loro Piana topcoats dreaming of what … a nice quiet prison? Their liability for this latest attempt to escape the whirlwind through forced pharmaceuticals and the construction of the Biomedical Security State, must be dawning on them. It was always a possibility, but they figured the populace — thanks to their equally witless behaviourists — were so dumb they’d consent to being permanently damaged and think it was the fault of the extreme right. And climate change.
[…]
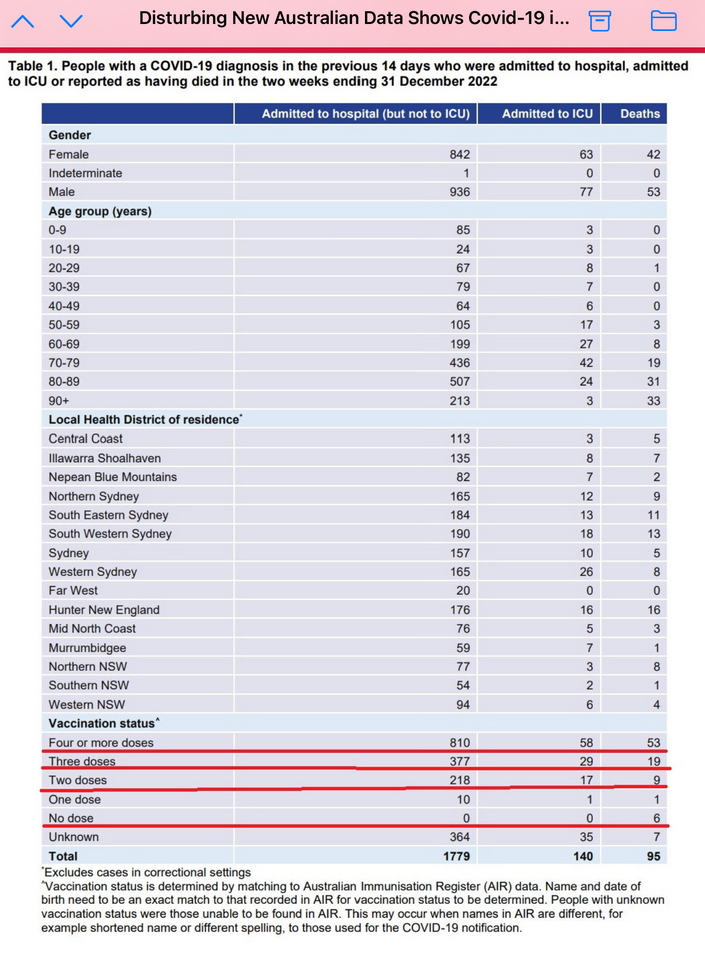
In Australia, the more Covid shots you’ve had, the more Covid you get and the more you die. The unvaccinated sail by relatively unperturbed.
Did you know that Big Pharma takes between $8 to $10 Trillion out of the US economy every year? GDP is only $23 Trillion. That’s a lot of money to claw back by every injured person, every family who lost a wage earner, a mother, a treasured child. This is a profit center for the great unwashed unmatched in human history. A massive transfer of wealth from the .01% to us.
They are all liable: every executive, every celebrity, every film producer, every hospital chief, every newspaper publisher, every television station owner, every multinational media company, every medical center, every university, every employer, every politician who forced and bullied people. Their wealth is about to become ours.

November 9, 2022
Liberal political fortunes ride “especially women in the suburbs of the Greater Toronto Area” … and those women are angry right now
In The Line, Ashley Csanady has some advice for Justin Trudeau in the lead-up to the next federal election that he really needs to pay attention to:
Poll after poll has told us the Liberals lost white male voters a long time ago, and their electoral fortunes, especially in Quebec and suburban Ontario, rely on women, especially women in the suburbs of the Greater Toronto Area. This isn’t to say dads and other caregivers aren’t angry. Families take many shapes and anyone with small people at home has faced the same indignities over the past nearly three years. However, politically and demographically, it’s the Ontario moms who are going to make or break the next election. And when folks are angry, it doesn’t matter who the incumbent is, they are wont to vote them out.
Nor is it not just about the children’s pain meds.
It’s about the fact we can’t find antibiotic eye drops over-the-counter either (a shortage one pharmacist told me is even worse than the one for pain and fever meds for the wee ones). Another shortage that means we must then turn to an already over-burdened health-care system to get a prescription for a medicine that may or may not be in stock.
Oh, and if that respiratory virus going around turns nasty, we aren’t even certain there will be a hospital bed for our babies when they need it most.
Then there is the infuriatingly slow roll-out of affordable childcare in this province. Parents once again caught between the feds and the province in a battle that may drag out the process so long that many expecting relief will see their kids off to junior kindergarten before it arrives.
Grocery bills are skyrocketing, and while I admit I’m privileged enough to absorb the eye-popping increases, so many families simply cannot. Imagine telling a picky toddler they can’t have their favourite snack because you can’t afford the crackers.
Now, Ontario moms had to deal with yet another disruption to their kids’ schooling, which threw their work lives into chaos once again. More disruptions are possible should bargaining fail again. This just after many women who left the workforce or took a step back from their careers during the pandemic were just getting back into the swing of things.
I made this point — that Ontario moms are angry and much of that anger is directed at political leaders, but I don’t expect it to fall on Ontario Doug Ford — on Twitter a couple weeks back. For this, I was “reminded” — more like chided — that many of these challenges are Mr. Ford’s fault. Or global challenges no logical person could blame the prime minister for. The partisans in my mentions were right on both counts. But here’s what they got wrong:
It doesn’t matter if I’m being “unfair” to Mr. Trudeau, because politics is unfair.
And as for Mr. Ford’s share of the blame, voters punish who’s up next at the ballot box, especially in a crisis. They had a chance to take out their rage on the PCs in June. They didn’t. So who does that leave up next?
October 20, 2022
QotD: “Medical gaslighting”
Of course, sometimes doctors will be wrong, because in my experience most of them are not great diagnosticians. And it will usually involve women because women visit doctors with complaints much more often than men. But “medical gaslighting” imports a notion of bad faith instead of error. It’s the medical version of “believe all women”, and you know how well that turned out …
Glenn Reynolds, Instapundit, 2022-07-17.
September 10, 2022
“Things have gone horribly wrong in American medicine; for example, ‘physicians are sharing ideas'”
Chris Bray on the American healthcare system’s descent into not just “rule by experts” — which you rather expect for a field like medicine — but the far worse “rule by government-approved experts”:
Our $3.7 trillion medical system is characterized by its fragility, the narrative says, with patients who can’t get treatment and doctors who can’t learn. So what’s gone wrong? Here’s the headline, with a whole universe of silly assumptions baked into every word:
Things have gone horribly wrong in American medicine; for example, “physicians are sharing ideas”.
I’m just taking a moment to stare at my own sentence. Be right back.
Anyway, medicine is broken — doctors are thinking. Sick people show up to see them, and they try to figure it out themselves by using, like, evidence and diagnostic practice and their medical knowledge. Lacking government directives, physicians are living with a horrible system in which they have to assess sick people and come up with their own answers about their illnesses and the best course of treatment. And so, Politico reports, networks of doctors are gathering to share data and work collaboratively, a sure sign that things have gone horribly wrong:
While the network is helping patients and doctors navigate the disease’s uncharted waters, long Covid doctors say there’s only so much they can do on their own. The federal government should be doing more, they say, to provide resources, coordinate information sharing and put out best practices. Without that, the doctors involved fear the condition, which has kept many of those afflicted out of the workforce, threatens to spiral.
Imagine what doctors will be like after two more generations shaped by the assumption that the federal government is the only proper source of “best practices”. The pathologization of socially and institutionally healthy behavior — professionals, confronted with a new problem, work together to gather evidence so they can analyze and apply it — speaks to the ruin inflicted by the pandemic, by the federal funding and steering of science, and by the Saint Anthonying of medicine: If government doesn’t tell you how, you can’t possibly know how. You expect your doctor to use a lifetime of education and experience to figure out what’s wrong with you; Politico expects your doctor to apply the government guidelines, but finds to its alarm that the government doesn’t offer any. How can you make a sandwich if the government hasn’t published a protocol on the application of condiments?
If you’ve felt rigidity and a lack of productive exchange in your conversations with your own doctor, we may have a suggestion here about the why part. I can’t assert that with total confidence, because the federal government hasn’t provided me with an analytical framework.
And so the debilitation of people who should have professional knowledge and competence becomes normal and expected. A scientist is someone who gets checks from the NIH, unless the scientist is one of the other kind and gets checks from the NSF, and ideological compliance is part of the deal. A doctor is someone who applies the government protocols. Federal agencies wear your doctors like a skin suit, and apply their medical solutions through the hands of others. If that’s not how it works — if your doctor works in creative and thoughtful ways to make sense of an illness and provide an effective treatment — something has gone wrong.

August 29, 2022
“Follow the science!”, “No, not like that!”
Chris Bray recounts his experiences when he “followed the science” over the Wuhan Coronavirus:
It’s happening again, and so is the response. It’s becoming our one persistent cultural cycle.
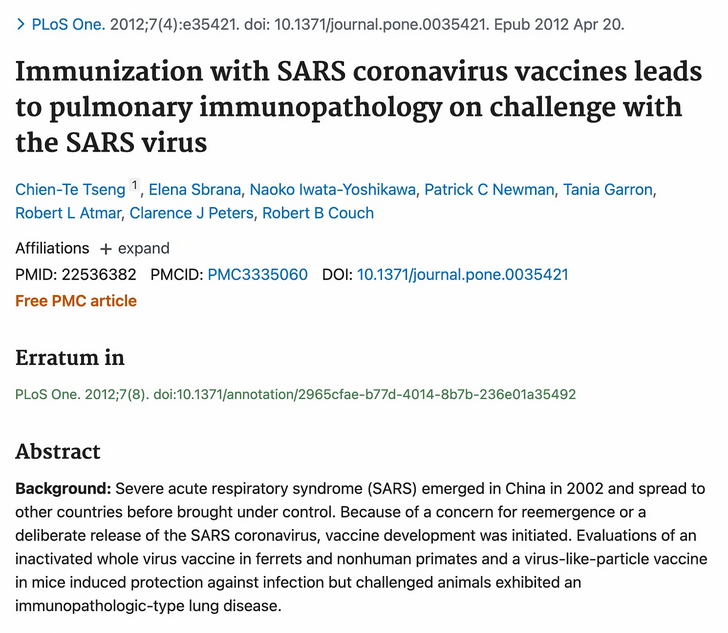
During the first availability of the Covid-19 “vaccines” — which don’t prevent transmission or infection, but we changed the meaning of that word, so shut up shut up shut up — I did what I usually do: I thought about the past to try to make sense of the present. If we’ve instantly produced safe and effective vaccines for SARS-CoV-2, I wondered, why didn’t we do the same for SARS-CoV-1? It took less than five minutes to answer that question:
So scientists did come up with a vaccine for SARS-CoV-1, but when they gave it to animals, it made the animals extremely susceptible to severe illness when they were “challenged” with the virus again — “suggesting hypersensitivity to SARS-CoV components was induced”. And so, the authors of that 2012 paper argued, “Caution in proceeding to application of a SARS-CoV vaccine in humans is indicated.”
Because I believe in science, I followed that advice, and I told my doctor that I was following that advice — and that I wasn’t terribly concerned about Covid-19 anyway, so whatever. I would be cautious about injecting a novel medical product into my body: I would wait, calmly. She assured me that there was no scientific shortcutting at all in the development of the vaccines for SARS-CoV-2, which were absolutely known to be 100% safe and effective, but she also agreed that there was nothing wrong with watching and waiting for a few months.
I meant it. At that point, I hadn’t refused the vaccines — I had just decided that I would wait for a bit to see how they played out once they’d been injected into a few billion human lab rats.
And then the shaming started. I was uninvited from a family event, and ordered to stay away — and then, after a short pause, repeatedly shamed by email as a disgusting selfish pig who made the family sick with my ignorance and selfishness. (Distant family, thankfully.) The public sphere came alive with this message, and Joe Biden let me know that his patience was wearing thin for my kind. Social media was a daily fear bath, and consumed with shaming rituals.
It was exactly that message that turned my skepticism, my preference for watching and waiting, into a flat and permanent refusal. People said they were talking about science — in a vicious flood of hyperemotional shaming language, the hysterical tone and substance of which made it clear that they weren’t talking about science at all. They were talking about their fearfulness and their weakness; they were talking about their cowardice, and about the shame they felt at finding their fear of the air wasn’t shared. The shaming made me contemptuous; it secured my commitment to resist.
So now comes a new flood of shaming messages, assuring people that mere political disagreement is a sure sign of monstrous cruelty and hate.
August 20, 2022
Yes, you will end up owing your conspiracy theorist friend an apology at this rate …
Chris Bray re-enacts a few of the minor erasures, walk-backs, and out-and-out lies coming from organizations who’ve spent the last two-plus years spreading a line of medical “truth” that, day-by-day, appears a bit less “truth-y” all the time:
I can’t get this attack on Dr. Ryan Cole out of my head:
What’s becoming very clear is that the narrative is going to shift by inches, eventually ending up at the place where mRNA dissenters started, but. Let’s get through the first part, and I’ll get to that but in just a moment. Look at, for example, the recent stealth-edit on the CDC website that quietly removed the assurance about the spike protein from mRNA injection leaving your body in a hurry. So on Monday it’s disinformation to falsely claim that the spike protein lingers in your body, and you’re a dangerous extremist if you say it; on Tuesday, the simple fact of lingering spike protein was always known and never contested. That’s DISINFORMA— hold on, I’ve just been handed a new memo.
This is going to keep happening, in little pieces that move toward reality. There are ZERO mRNA deaths, you lying idiots, and you need to stop spreading disin— uh, hold on, it says here that, uh …
In a year, or in five years, the things that Ryan Cole and Clare Craig and Peter McCullough and Tracy Beth Hoeg and Robert Malone and all the other MONSTERS have been saying will be validated and acknowledged. We’ll know that the mRNA injections caused heart damage and a cancer spike, and we’ll know that mRNA-injected people get sick more often than the dirty unvaccinated. Look at the matter-of-factness with which Deborah Birx says that oh yeah, I always knew these vaccines — vaccines! — weren’t going to prevent infection. A year before she shrugged and said she’d always known that, you would have lost your social media accounts for saying exactly what she just said. Yesterday’s idiotic conspiracy theory disinformation nonsense is today’s “yeah, we always knew that”.
Now, here’s my big but: The narrative is going to turn, in a long series of tiny and unacknowledged shifts, until it matches what the heretics have always been saying — but my bet is that the heretics will not be rehabilitated. Ryan Cole, to stick with the opening example, will be proven correct, but he will not be vindicated. The YOU CAN’T SAY THAT, IT’S DISINFORMATION oh wait it’s totally true maneuver doesn’t rehabilitate the crimethinkers. You can think X when it’s time to think X; if you think X too early, you remain a thought criminal.
The truthtellers in medicine will be proved correct, but they’ll still be resented and excluded.



