Unlike most other Anglosphere countries, Canada does not have a resurgent right wing in domestic politics — we barely have a right wing at all — and the governing Liberal Party is constantly trying to steal sitting opposition MPs to achieve a majority of seats in Parliament. It’s no wonder that Alberta’s separatist movement has been active the last few years. In case you still have an optimistic view of Canada’s present and future, here’s a long “state of Canada” post from John Carter that will probably increase the numbers signing up for free euthanasia (“MAID” in Canadian):
The US is now leading Canada 3-0 in international hockey. If you count the Stanley Cup as an occasional international match, a Canadian team hasn’t won since 1993. For a country that has long practically defined itself as the Hockey Nation, this is especially humiliating. Given the continual year-round repetition of the Elbows Up mantra, this is the kind of thing a Roman augur would have interpreted as a portent of divine disfavour.
Months, you say? Oh dear.
Consistent with that interpretation, Canada’s recent humiliations have not been limited to sportspuck losses. What follows is a snapshot in time, headlines from a country beset by interlocking economic, demographic, spiritual, and political crises, a country which has not had good news in so long that it has forgotten what optimism even looks like.
Item: Canada recently watched the worst school shooting in Canadian history, and the second-worse mass shooting after the infamous 1989 Montreal Massacre in which “Mark Lepine”1 shot 14 female engineering students. The shooting took place in Tumbler Ridge, British Columbia, a small rural village in the country’s north, and claimed the lives of 10 people including the shooter, his mother, his brother, and several students. Dozens of others were injured. It soon turned out that the murderer was a trannie whose brain had been twisted into a psychotic pretzel by psychedelics, legal weed, SSRIs, and the gender woo he was force-fed at school, at home, and on Reddit. This has led to it being referred to as the Tumblr Shooting. Naturally, both the Royal Canadian Mounted Police and the Canadian media went out of their way to respect the shooter’s pronouns in all reporting and official communications. The media even made sure to give the shooter an AI filter glow-up, so that he could be remembered as the pretty girl we all know he really was deep down inside.
After a desultory and hilariously unsuccessful attempt at scolding the public that the problem wasn’t trannies, but guns or whiteness or something (blessedly, they couldn’t say “men” this time), the Canadian media just dropped it, though not before the government flew the flag at half mast.
Which is how this happened.
Item: A former school board trustee in Chilliwack, British Columbia, was fined $750,000 for failure to respect pronouns. Shooting up a school is bad, but misgendering is unforgivable.
[…]
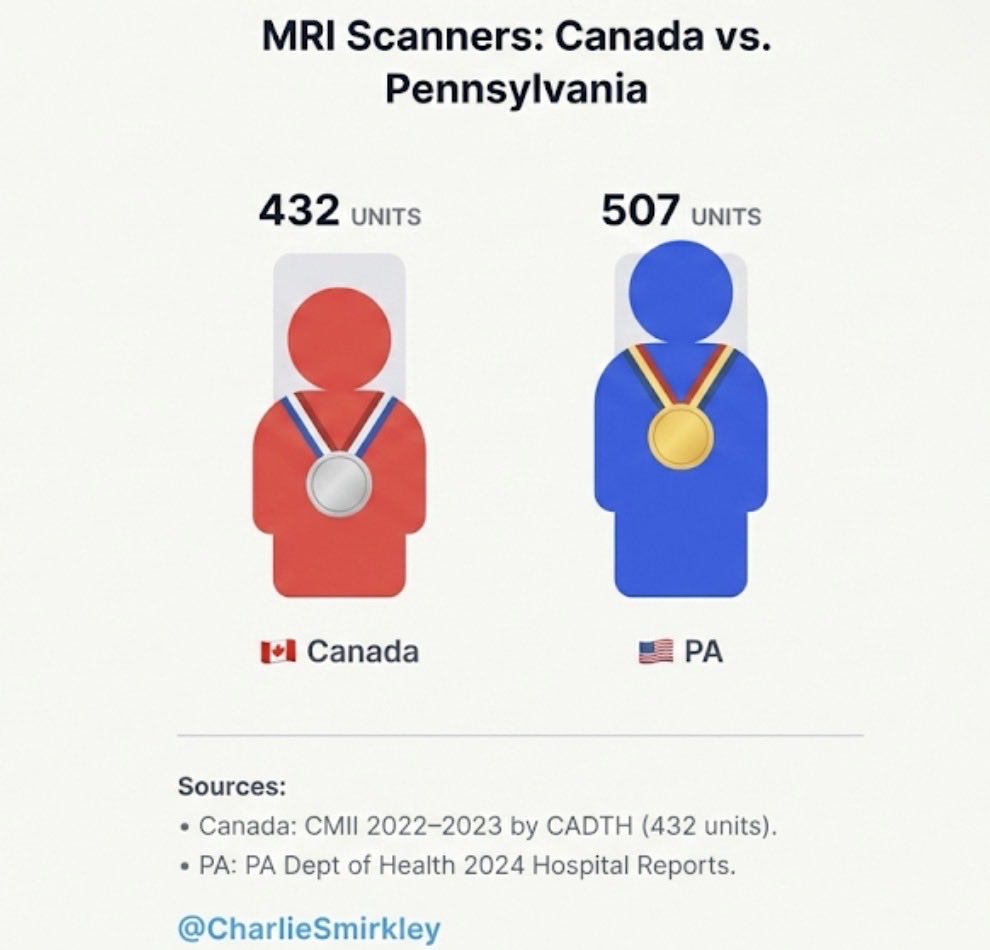
Item: A xeet went viral in which a leaflib tried to fact check an American poster making fun of 18-month MRI wait times by pointing out that she’d only had to wait six months, prompting widespread mockery from incredulous Yanks.
Pennsylvania, which has about 1/3 of Canada’s population, has more MRIs than all of Canada put together. The Canadian mind cannot comprehend, etc.
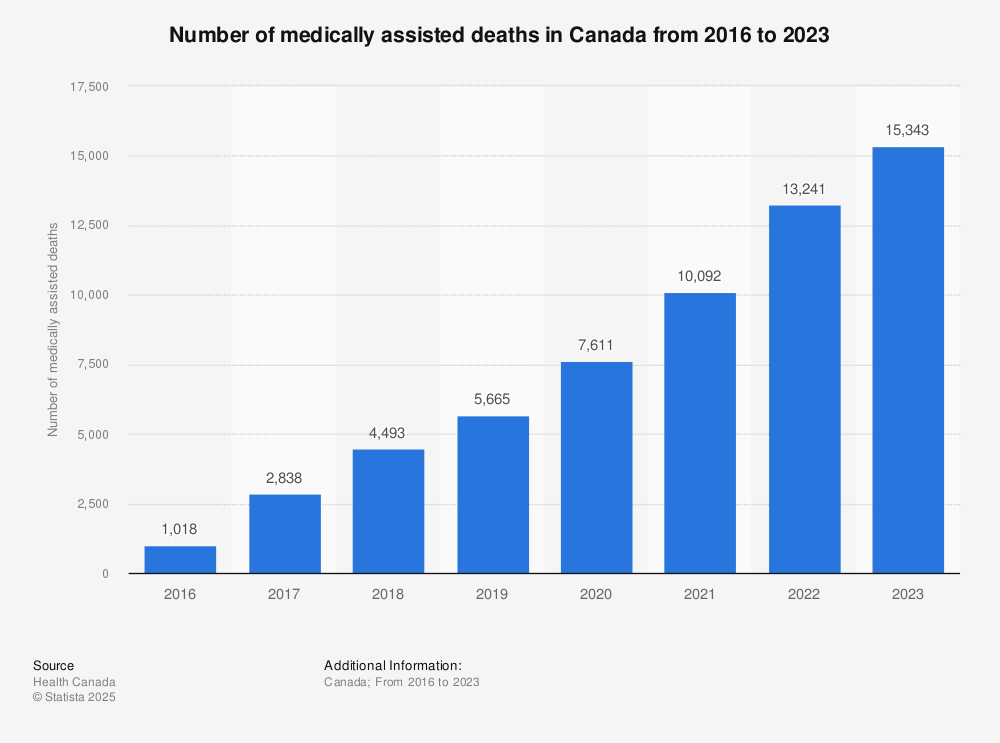
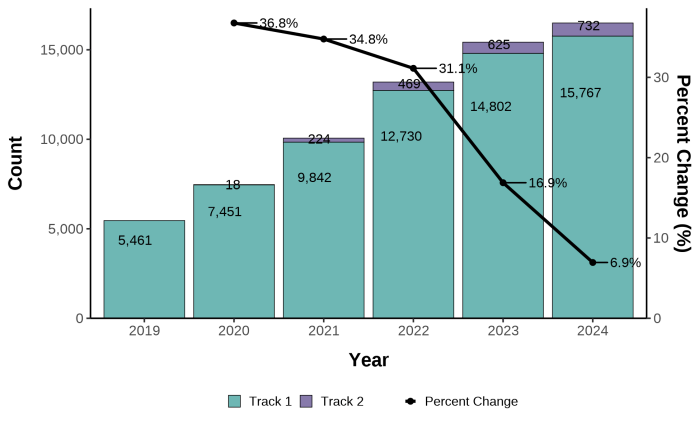
Item: Euthanasia via Canada’s Medical Assistance in Dying (MAiD) program now accounts for 1 death in 20 in Canada. The overwhelming majority, around 96%, of MAiD recipients are white, despite white Canadians comprising 86% of Canadians in the elderly demographic that dominates assisted suicide participants.
Since 2016 over 76,000 Canadians have been killed by MAiD. Moreover, the program is accelerating: the death toll in 2024 was the highest on record at 16,499. Annual death tolls have risen by around a few thousand every year since the program started, with no sign of stopping. Canada is expected to hit 100,000 MAiD deaths by summer.
Item: While most MAiD victims are elderly and infirm, this is not true in every case. Recently it came out that a 26-year-old man was euthanized, simply because he was depressed over his diabetes-induced blindness. His family allege that he doctor-shopped until he found one who would kill him (she has apparently killed several hundred others).
MAiD was originally billed as an easy, painless out for people with terminal illnesses, a dignified death that would spare them a few months of pointless agony. It’s now being extended to people whose imminent death is not reasonably foreseeable. Several Canadian Armed Forces veterans have been offered MAiD in lieu of treatment for injuries sustained in the course of their service.
The primary goal of MAiD is almost certainly to reduce pressure on Canada’s overstretched public health care system whilst simultaneously reducing the fiscal burden of pensioners on the federal budget. Someone looked at the financials, and concluded that unfunded liabilities were going to bankrupt the country when the boomers reached their 80s. Therefore the government is talking them into killing themselves. However, while they’re at it, they might as well expand the program to hasten demographic replacement within the younger sectors of the population pyramid.
- Née Gamil Gharbi, a detail the Canadian media successfully kept from us for decades as it didn’t fit their narrative that “men” are the problem, rather than men from … certain places.