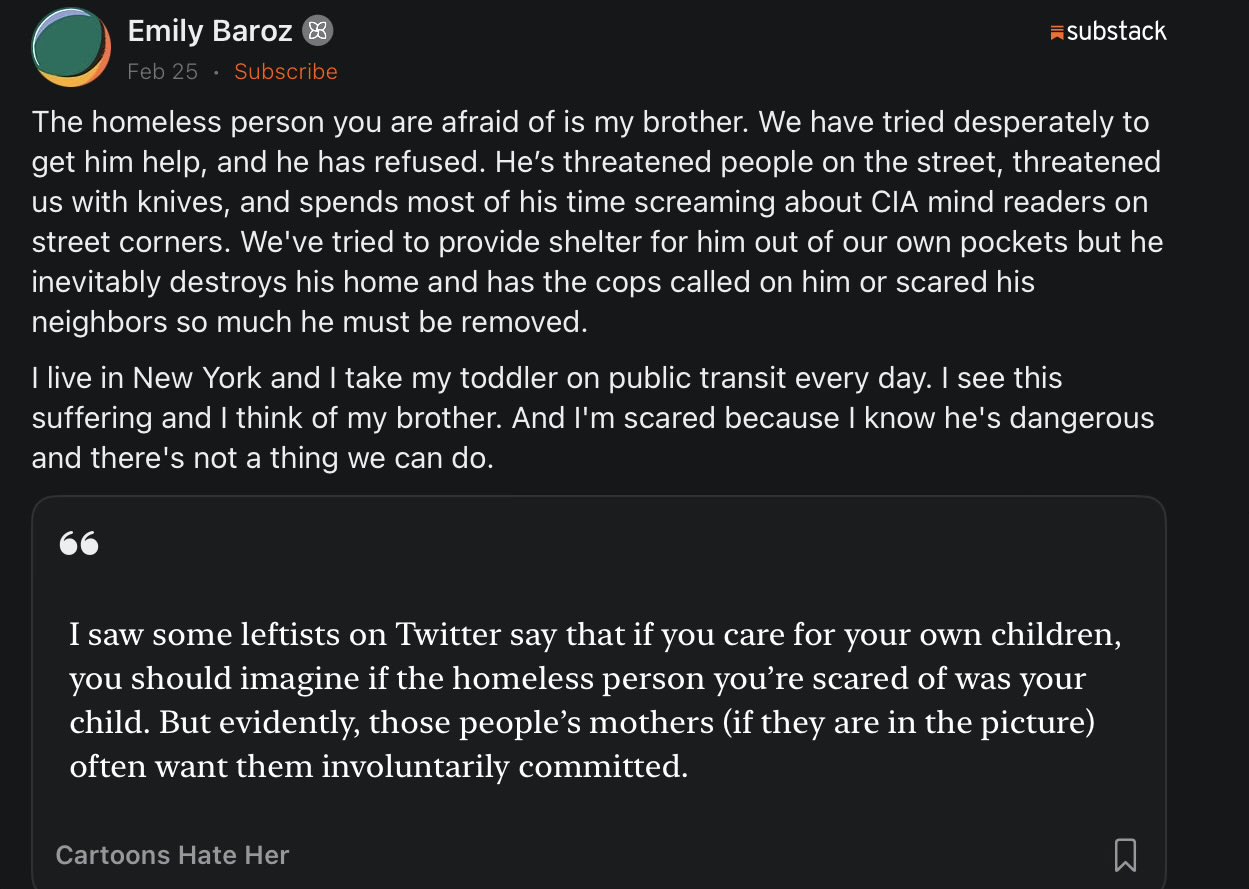
On the social media site formerly known as Twitter, L. Wayne Mathison responds to someone explaining their family’s tragic problem of a homeless relative:
The post hits a nerve because it exposes the part of the homelessness debate people prefer not to talk about.
A lot of the public story says homelessness is mainly about housing and compassion. If we build more units and remove stigma, the problem fades. That sounds humane. The trouble is that it ignores what families dealing with severe addiction and psychosis actually face.
Emily Baroz describes the reality many relatives know too well. The person on the street is often not just poor. They are deeply mentally ill, addicted, paranoid, sometimes violent, and frequently refusing help. Families try everything. Housing. Money. Treatment. Support. The illness itself destroys the ability to cooperate. Meanwhile the legal system often blocks intervention until someone gets hurt.
So the public debate becomes strange theatre. Compassion is defined as leaving the person alone. Authority is treated as cruelty.
That brings us closer to home. Manitoba’s NDP government is now moving toward supervised consumption sites. The argument is harm reduction. The idea is that if people are going to use drugs anyway, the state should at least make it safer.
The problem is that the evidence across Canada is far from comforting. Vancouver, Toronto, and other cities expanded harm-reduction sites over the last decade. Yet overdoses, street disorder, and visible addiction kept rising. Recovery rates did not suddenly surge. In many neighbourhoods the result was more normalization of drug use without a clear path back to stability.
If a policy is supposed to reduce harm, the basic question is simple: are fewer people addicted, dying, or trapped in the street?
If the answer is no, the policy deserves scrutiny.
Safe consumption sites may prevent some immediate overdoses. But they also risk locking people into a long-term cycle where the system manages addiction instead of helping people escape it. Families who are begging for treatment beds, detox spaces, psychiatric care, and recovery programs often watch governments invest more energy in enabling use than in ending it.
That’s the tension people feel but rarely say out loud.
A compassionate society does not abandon people to addiction while calling it care. Compassion sometimes means structured treatment, involuntary intervention when someone is clearly incapable of making rational choices, and serious investment in recovery infrastructure.
Otherwise we are simply managing decline.
And families like the one in that post already know it.