At Founding Questions, Severian discusses how our understanding of what we now label “Post-Traumatic Stress Disorder” evolved from how doctors visualized bodily ailments over a century ago:
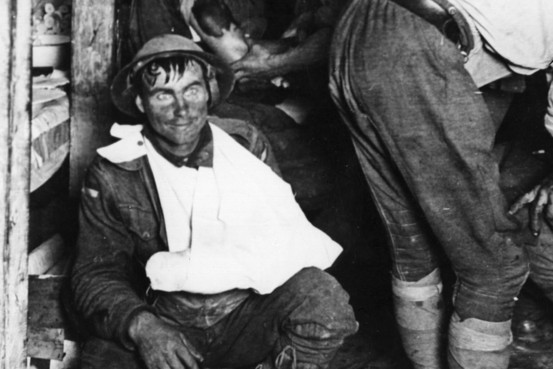
A shell-shocked and physically wounded soldier in the First World War.
I mentioned “shell shock” yesterday, so let’s start there. Medicine in 1914 was still devoted to the “Paris School,” which assumed nothing but organic etiology for all syndromes. Sort of a reverse Descartes — as Descartes (implicitly) “solved” the mind-body problem by disregarding the body, so the “Paris School” of medicine solved it by disregarding the mind. So when soldiers started coming back from the front with these bizarre illnesses, naturally doctors began searching for an organic cause. (That’s hardly unique to the Paris School, of course; I’m giving you the context to be fair to the 1914 medical establishment, whose resistance to psychological explanations otherwise seems so mulish to us).
They’d noticed something similar in the late 19th century, with industrial accidents and especially train crashes. When a train crashed, the people in the first few cars were killed outright, those in the next few wounded, but the ones in the back were often physically fine. But within a few hours to weeks, they started exhibiting all kinds of odd symptoms. Hopefully you’ve never been in a train crash, but if you’ve ever been in a fender-bender you’ve no doubt experienced a minor league version of this.I hit a deer on the highway once. Fortunately I was at highway speed, and hit it more or less dead on (it jumped out as if it were committing suicide), so it got thrown away from the car instead of coming through the windshield. The car’s front end was wrecked, naturally, but I was totally fine. I don’t think the seatbelt lock even engaged, much less the airbag, since I didn’t even have time to hit the brakes.
The next few hours to days were interesting, physiologically. It felt like my body was playing catch up. I had an “oh shit, I’m gonna crash!!!” reaction about 45 minutes after I’d pulled off to the side of the road, duct-taped the bumper back on as best I could, and continued to my destination. All the stuff I would have felt had I seen the deer coming came flooding in. Had I not already been where I was going, I would’ve needed to pull over, because that out of the blue adrenaline hit had my hands shaking, and my vision fuzzed out briefly.
The next morning I was sore. I had all kinds of weird aches, as if I’d just played a game of basketball or something. I assume part of it actually was the impact — it didn’t feel like much in the moment, but if it’s enough to crumple your car’s front end (and it was trashed), it’s enough to give you a pretty good jolt. That would explain soreness in the arms, elbows, and shoulders — a stiff-armed, white-knuckle grip on the steering wheel, followed by a big boom. But I was also just kinda sore all over, plus this generalized malaise. I felt not-quite-right for the next few days. Nothing big, no one symptom I can really put my finger on, but definitely off somehow — a little twitchy, a little jumpy, and really tired.
Having done my WWI reading, I knew what it was, and that’s when I really understood the doctors’ thought processes. I really did take some physical damage, because I really did receive a pretty good full-body whack. It just wasn’t obvious to the naked eye. And since everyone has experienced odd physical symptoms from being rattled around, or even sleeping on a couch or sprung mattress, it makes sense — the impact obviously jiggled my spine, which probably accounts for a great many of the physical symptoms. Hence, “railway spine”. And from there, “shell shock” — nothing rattles your back like standing in a trench or crouching in a dugout as thousands of pounds of high explosive go off around you. It must be like going through my car crash all day, every day.
Skip forward a few decades, and we now have a much better physiological understanding of what we now call (and I will henceforth call) Post-Traumatic Stress Disorder (PTSD). There’s a hypothesis that I personally believe, that “shell shock” is also a whole bunch of micro-concussions as well as “classic” PTSD, but let’s leave that aside for now. The modern understanding of PTSD is largely about chemistry. Cortisol and other stress chemicals really fuck you up. They have systemic physical and mental effects. If those chemicals don’t get a chance to flush out of your system — if you’re in a trench for weeks on end, let’s say — the effects are cumulative, indeed exponential.
Returning to my car crash: I was “off” for a few days because my body got a huge jolt of stress chemicals. That odd not-quite-right thing I felt was those chemicals flushing through. Had I gone to a shrink at that moment, he probably would’ve diagnosed me with PTSD. But I didn’t have PTSD. I had a perfectly normal physiological reaction to a big shot of stress chemicals. If I’d gotten into car crash after car crash, though, day in and day out, that would’ve been PTSD. I’d be having nightmares about that deer every night, instead of just the once. And all that would have cumulative, indeed exponential, effects.
He then goes on to cover similar physical reactions to stimuli in modern life, so I do recommend you RTWT.