
I question the idea that modern life has increased the total amount of lunacy in the world. Thanks to the Internet in general, and social media in particular, the volume of the world’s lunatic population has been amped well past 11 … but I think this is less a case of “Twitter creating lunatics” than “online anonymity letting people fly their freak flags openly”. Deliberately avoiding sex and politics, an example: On a road trip recently, I started flipping channels in my hotel room, and I came across a show called Dr. Pimple Popper. I swear, this is absolutely a real thing that exists. Here’s this woman, a dermatologist I guess, rooting around in cysts and boils and tumors and whatnot for the cameras, and … that’s it.
Not only is there an audience for this — which I never would’ve believed — there’s enough of an audience for it that it’s on basic cable. See what I mean? Somehow, the marketing guys determined that yes, there are enough people out there who want to see cysts being cauterized that we can make an entire show out of it. How could they figure it out? Beats me, but unless some suits at TLC had a contest to see what’s the silliest, grossest thing they could actually get broadcast, I’m betting that there was a group of Internet weirdos out there discussing it, and the marketing boys just ran with it.
Applying that to the topic at hand, my guess is that, since it’s so easy for people to be Massively Online these days, the kind of folks with that particular type of mental problem pretty much live on Twitter, where — as anyone who has waded into that cesspit for more than five minutes knows — the Twitterati absolutely cannot distinguish “talking about doing something” from “actually doing something”.
Severian, “Friday Mailbag”, Rotten Chestnuts, 2021-06-04.
July 3, 2024
June 10, 2024
The FDA has a jaundiced view of psychotherapy involving the use of MDMA (aka “Ecstasy”)
Colby Cosh indulges in a minor “I told you so” after the FDA’s expert panel recommended against the agency permitting any medical use of MDMA, despite some experiments indicating it does have therapeutic value:
Ball-and-stick model of the 3,4-methylenedioxy-methamphetamine molecule, also known as MDMA, or ecstasy, a well-known psychoactive drug. Based on the crystal structure of MDMA hydrochloride, as determined by X-ray diffraction.
Color code: Carbon, C: black, Hydrogen, H: white, Oxygen, O: red, Nitrogen, N: blue.
Image by Jynto via Wikimedia Commons.
Hopes for research into therapeutic uses of psychedelic drugs received a setback last week, one that your correspondent saw tripping (geddit?) up the road in advance. An expert panel published its official advice to the United States Food and Drug Administration (FDA) on permitting medical use of MDMA, the synthetic nightclub enhancer that we’re afraid the kids probably still aren’t calling “ecstasy” or “molly”.
There is long-recognized potential for MDMA to be combined with classical psychotherapy in treating emotional disorders, notably post-traumatic stress (PTSD), and now there are some small, limited studies showing evidence of positive effects.
But the FDA’s scientists weren’t very impressed with this evidence, and they voted almost unanimously against creating a therapeutic exception to the illegality of ecstasy, which the U.S. Controlled Substances Act classifies as a “Schedule 1” drug, right next to heroin. The panel’s advice isn’t binding on the agency, which is crawling in somewhat good faith toward recognizing the understudied medical potential of psychedelics. But the vote emphasizes the inherent problems that drugs face, once they are defined in law as “recreational”, in winning over skeptical scientists.
Reason magazine’s great drug-war correspondent Jacob Sullum has a thorough discussion of the issues. The existing research, despite some impressive headline results, has garden-variety issues with dropout rates, follow-ups and occasional researcher shenanigans. But the big problem, which defies easy technical solution, is with scientific blinding of the research subjects.
Scientific trials of the modern kind are predicated upon separating illusory placebo effects from genuine treatment effects. Researchers expect that a high-quality study will have a control group that receives sham treatment or none at all, and good practice requires that experimenters and their guinea pigs are both blind to who is in what group.
News flash: most people can tell whether they’ve been really given a psychedelic drug. Indeed, most doctors can tell whether they’ve given a patient a genuine psychedelic drug, and how much of it. Many placebo-controlled trials on psychoactive drugs, perhaps most of them, thus suffer from an alleged problem of broken blinding. (Have a glance, for example, at Table 2 in this review of blinding procedures in psychedelic studies.)
June 5, 2024
QotD: Mental health at “Flyover State”
Given that, and given how lunatic professors’ actual beliefs are, there’s pretty much nothing you can’t get away with saying in the ivory tower if you play your cards right. In much the same way Jon Stewart rode his “clown nose on / clown nose off” act to adulation from the smart set, you can say whatever you want if you keep it ambiguously crazy. (You know how it goes — if you agree with Stewart, he’s doing straight political commentary; but if you disagree with him to the point where he might lose sponsors, c’mon man, he’s just a tv comedian).
I’ll give you an example. Back in 2008, during the Democratic primaries, it was all the rage on campus to be anti-Obama. You’ll just have to trust me on that, I guess, but if you believed my previous “inside the ivory gulag” posts, I’m sure you’ll understand why that fad existed — everyone’s playing the “more radical than thou” game, and what’s more radical than being against the black guy, because his positions are such weak sauce Liberal boilerplate? The real People’s Candidate back then was Dennis Kucinich, and if normal people remember anything about him, it’s that he was more than a little Fox Mulder-y on the question of extraterrestrial life.
Anyway, whenever anyone asked me who I was voting for, I’d give Obama both barrels, always from the most extreme conservative position … but when I noticed the SJW I was talking to had finally cottoned to that, I ended with something like “And what’s worst is that unlike some candidates, Obama refuses to take the saucer people menace seriously!!”
Severian, “Friday Mailbag”, Rotten Chestnuts, 2021-06-04.
May 22, 2024
Scott Alexander reviews The Others Within Us
At Astral Codex Ten, Scott Alexander discusses teh new hawtness in psychotherapy as expounded in Robert Falconer’s new book The Others Within Us:
Internal Family Systems, the hot new1 psychotherapy, has a secret.
“Hot new psychotherapy” might sound dismissive. It’s not. There’s always got to be one. The therapy that’s getting all the buzz, curing all the incurable patients, rocking those first few small studies. The therapy that was invented by a grizzled veteran therapist working with Patients Like You, not the out-of-touch elites behind all the other therapies. The therapy that Really Gets To The Root Of The Problem. There’s always got to be one, and now it’s IFS.
Sufficiently new and popular therapies are hard to get. Therapist training starts slow – the founder has to train the second generation of therapists, the second generation has to train the third generation, and so on. IFS says they have a 10,000 person wait list for their training program. So lots of people have heard great things about IFS, maybe read a manual or two, but never tried it or met anyone who has.
What I gather from the manuals: IFS is about working with “parts”. You treat your mind as containing a Self — a sort of perfect angelic intellect without any flaws or mental illnesses — and various Parts — little sub-minds with their own agendas who can sometimes occlude or overwhelm the Self. During therapy, you talk to the Parts, learn their motives, and bargain with them.
For example, you might identify a Part of you that wants to sabotage your relationships. You will visualize and name it — maybe you call her Sabby, and she looks like a snake. You talk to Sabby, and learn that after your first break-up, when you decided you never wanted to feel that level of pain again, you unconsciously created her and ordered her to make sure you never got close enough to anyone else to get hurt. Then you and the therapist come up with some plan to satisfy Sabby — maybe you convince her that you’re older now, and better able to deal with pain, and you won’t blame her if you get close to someone and have to break up again. Then you see a vision of Sabby stepping aside, maybe turning off the Windmill Of Relationship Sabotage or something like that, and then you never sabotage your relationships again. It’s more complicated than that, but that’s the core.
All of this is the classic version everyone learns from the manual. Before we get to the secret, let’s examine two big assumptions in more detail.
First, this isn’t supposed to be just the therapist walking you through guided imagery, or you making up a story you tell yourself. The therapist asks you “Look inside until you find the part that’s sabotaging your relationship”, and you are supposed to discover — not invent, discover — that your unconscious gives it the form of a snake called Sabby. And you are supposed to hear as in a trance — again, not invent — Sabby telling you that she’s been protecting you from heartbreak since your last breakup. When you bargain with Sabby, it’s a two-way negotiation. You learn — not decide — whether or not Sabby agrees to any given bargain. According to Internal Family Systems (which descends from normal family systems, ie family therapy where the whole family is there at once and has to compromise with each other), all this stuff really is in your mind, waiting for an IFS therapist to discover it. When Carl Jung talked about interacting with the archetypes or whatever, he wasn’t being metaphorical. He literally meant “go into a trance that gives you a sort of waking lucid dream where you meet all this internal stuff”.
(After reading the IFS manuals, I tried most of their tricks for initiating this sort of trance and meeting Sabby or whoever. I got nothing. I notice most of the patients with great results are severely traumatized borderlines, ie the same people who often get multiple personality disorder after the slightest hint from a therapist that this might happen. We’ll get back to this analogy later.)
The second assumption is that everything inside your mind is part of you, and everything inside your mind is good. You might think of Sabby as some kind of hostile interloper, ruining your relationships with people you love. But actually she’s a part of your unconscious, which you have in some sense willed into existence, looking out for your best interests. You neither can nor should fight her. If you try to excise her, you will psychically wound yourself. Instead, you should bargain with her the same way you would with any other friend or loved one, until either she convinces you that relationships are bad, or you and the therapist together convince her that they aren’t. This is one of the pillars of classical IFS.
The secret is: no, actually some of these things are literal demons.
1. Some people object to me calling it “new” – it was developed in the 1980s, and has been popular since the early 2010s. Still, the therapy landscape shifts slowly, and even an exponentially-growing therapy takes a long time to get anywhere.
April 30, 2024
TikTok for Tots (and Instagram, and Facebook, and Twitter, and …)
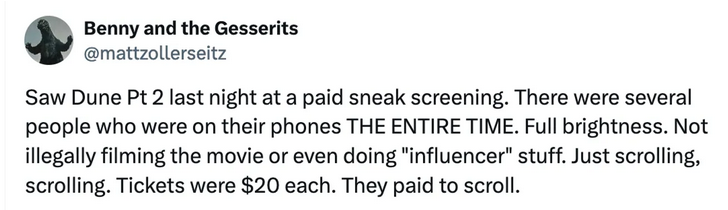
Ted Gioia has some rather alarming information on just how many kids are spending a lot of time online from a very early age:
The leader in this movement is TikTok. But the other major platforms (Instagram, Twitter, Facebook, YouTube, etc.) are imitating its fast-paced video reels.
My articles have stirred up discussion and debate—especially about the impact of slot machine-ish social media platforms on youngsters.
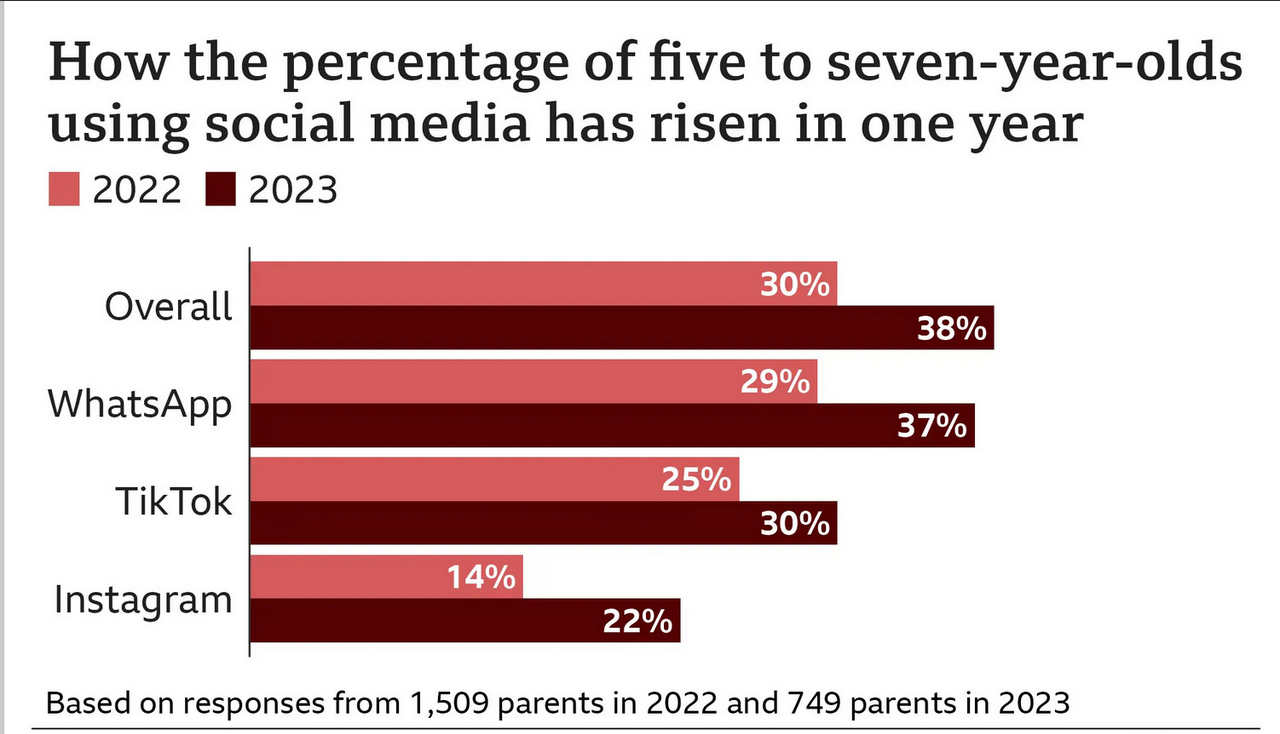
So I decided to dig into the available data on children and social media. And it was even worse than I feared.
30% of children ages 5 through 7 are using TikTok — despite the platform’s policy that you can’t sign up until age 13.
The story gets worse. The numbers are rising rapidly — usage among this vulnerable group jumped 5% in just one year.
By the way, almost a quarter of children in this demographic have a smartphone. More than three-quarters use a tablet computer.
These figures come from Ofcom, a UK-based regulatory group. I’ll let you decide how applicable they are to other countries. My hunch is that the situation in the US is even worse, but that’s just an educated guess based on having lived in both countries.
What happened in 2010?
One thing is certain — the mental health of youths in both the US and UK is deteriorating rapidly. There are dozens of ways of measuring the crisis, but they all tell the same tragic story.
Something happened around 2010, and it’s destroying millions of lives. […]
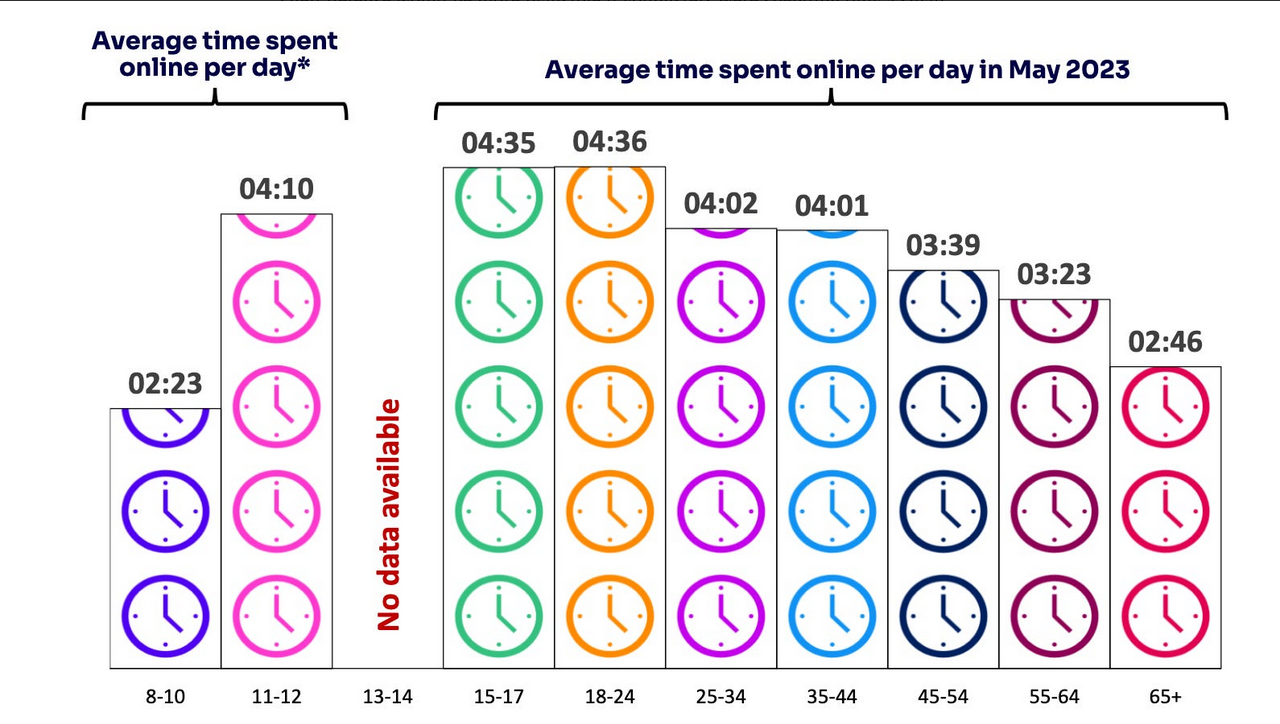
As early as age 11, children are spending more than four hours per day online.
Here’s a comparison of time spent online by age. Even before they reach their teens, youngsters are spending more than four hours per day staring into a screen.
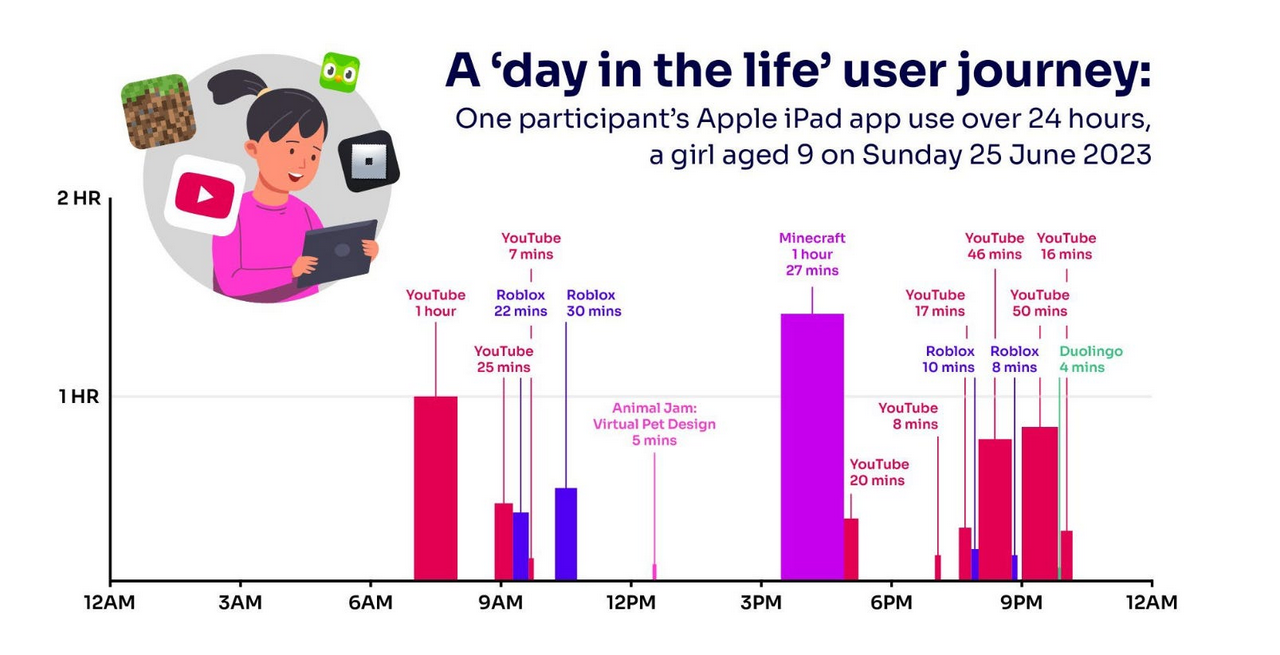
Here’s what a day in the digital life of a typical 9-year-old girl looks like.
I don’t find any of this amusing. But if you’re looking for dark humor, I’ll point to the four minutes spent on the Duolingo language training app at the end of the day. This provides an indicator of the relative role of learning in the digital regimen on the rising generation.
April 17, 2024
QotD: The mid-life crisis, male and female versions
Which is why I’ve found the COVID overreaction so bizarre. Realizing your own mortality changes things. You can always tell, for instance, when it has happened to a younger person — when they come home, combat vets often act like middle-aged men going through a midlife crisis. Readjustment to civilian life is hard. Read the great war narratives, and it’s clear that none of them ever really “got over it”. Robert Graves and Ernst Junger, for instance, both lived to ripe old ages (90 and 103, respectively), and were titans in fields far removed from battle … and yet, the war WAS their lives, in some way we who haven’t been through it will never understand, and it comes through in every line they wrote.
If the Covidians were really freaking out about COVID, then, I’d expect one of two broad types of reaction: Either party-hearty midlife crisis mode, or a new determination to get on with whatever’s left of life. Obviously neither of those are true, and I just can’t grasp it — these might be your last few weeks on Earth, and that’s how you’re going to spend them? Sitting in your apartment like a sheep, wearing a mask and eating takeout, glued to a computer screen?
If you want a measure of just how feminized our society has become, there you go. Call this misogyny if you must, but it’s an easily observed fact of human nature — indeed, it has been observed, in every time, place, and culture of which we have knowledge — that post-menopausal women go a bit batty. Though a man might know for certain that he dies tomorrow, he can still keep plugging away today, because he’s programmed to find real meaning in his “work” — we are, after all, running our snazzy new mental software over kludgy old caveman hardware.
Women aren’t like that. They have one “job”, just one, and when they can’t do it anymore, they get weird. In much the same way high-end sports cars would cease to exist if middle aged men ceased to exist, so there are entire aspects of culture that don’t make sense in any other way except: These are channels for the energies of post-menopausal, and therefore surplus-to-requirements, women. You could go so far as to say that pretty much everything we call culture — traditions, history, customs — exist for that reason. Women go from being the bearers, to being the custodians, of the tribe’s future.
Severian, “Life’s Back Nine”, Rotten Chestnuts, 2021-05-11.
April 9, 2024
Historical examples of social contagion
Andrew Doyle discusses how social contagions of the past resemble the current gender identity boom among western young people:

… social contagions are especially common among teenage girls, and that there are numerous historical precedents for this. I have written elsewhere about the Salem witch trials of 1692-93, in which a group of girls began seeing demons in the shadows and accusing members of their own community of being in league with the Devil. Then there were the various “dancing plagues” of the middle ages which seemed to impact young women in particular. In 1892, girls at a school in Germany began to involuntarily shake their hands whenever they performed writing exercises. And when I visited Sweden last year, I was told about a local village where, during the medieval period, the girls all inexplicably began to limp.
It’s perfectly clear that the latest social contagion to take hold in the western world is that of girls identifying out of their femaleness, either through claims that they are trans or non-binary. Whereas in 2012, there were only 250 referrals (mostly boys) to the NHS’s Gender Identity Development Service (GIDS), by 2021 the figure had risen to more than 5,000 (mostly female) patients. Gender activists like to claim that this is simply the consequence of more people “coming out” as society becomes more tolerant, and at the same time insist that it has never been a worse time to be trans. Consistency is not their strong suit.
Of course there are no easy answers as to the explosion of this latest fad, but surely the proliferation of social media has something to do with it. Platforms such as TikTok are replete with activists explaining to teenagers that their feelings of confusion are probably evidence that they have been “born in the wrong body”. For pubescent girls who are uncomfortable with their physiological changes, as well as sudden unwanted male sexual attention, the prospect of identifying out of womanhood makes complete sense. These online pedlars have some snake-oil to sell. And while a limping epidemic in a medieval village would be unlikely to spread very far, social contagions cannot be so confined in the digital age.
Much of this is reminiscent of the recovered memory hysteria of the late twentieth-century, when therapist cranks promoted the idea that most victims of sexual abuse had repressed their traumatic memories from childhood. It led to numerous cases of people imagining that they had been abused by parents and other family members, and many lives were ruined as a result. One of the key texts in this movement was The Courage to Heal (1988) by Ellen Bass and Laura Davis, which made the astonishing and unevidenced claim that “if you are unable to remember any specific instances … but still have a feeling that something abusive happened to you, it probably did”.
A common feature of social contagions is that they depend upon the elevation of intuition over material reality. Just as innocent family members were accused of sexual abuse because of “feelings” teased out by unscrupulous therapists, many girls are now being urged by online influencers to trust the evidence of their emotions and accept a misalignment between their body and their gendered soul. We are not talking here about the handful of children who suffer from gender dysphoria, but rather healthy children who have been swept up in a temporary craze.
April 5, 2024
“[T]oo many charlatans of this species have already been allowed to make vast fortunes at the expense of a gullible public”
Colby Cosh on his “emerging love-Haidt relationship” as Jonathan Haidt’s new book is generating a lot of buzz:
If Haidt has special expertise that wouldn’t pertain to any well-educated person, I wonder a little in what precise realm it lies. Read the second sentence of this article again: he’s a psychologist … who teaches ethics … at a business school? Note that he seems to have abandoned a prior career as an evolutionary biology pedlar, and the COVID pandemic wasn’t kind to his influential ideas about political conservatives being specially motivated by disgust and purity. Much of The Anxious Generation is instead devoted to trendy findings from “neuroscience” that it might be too kind to describe as “speculative”. (I’ll say it again until it’s conventional wisdom: a “neuroscientist” is somebody in a newly invented pseudofield who couldn’t get three inches into the previously established “-ology” for “neuro-“.)
These are my overwhelming prejudices against Haidt; and, in spite of all of them, I suspect somebody had to do what he is now doing, which is to make the strongest available case for social media as a historical impactor on social arrangements and child development. Today the economist/podcaster Tyler Cowen has published a delightfully adversarial interview with Haidt that provides a relatively fast way of boning up on the Haidt Crusade. Cowen belongs to my pro-innovation, techno-optimist, libertarian tribe: we both feel positive panic at the prospect of conservative-flavoured state restrictions on media, which are at the heart of the Haidt agenda.
But reading the interview makes me somewhat more pro-Haidt than I would otherwise be (i.e., not one tiny little bit). On a basic level, Cowen doesn’t, by any means, win the impromptu debate by a knockout — even though he is one of the most formidable debaters alive. Haidt has four key reforms he would like to see implemented politically: “No smartphones before high school; no social media before age 16; phone-free schools; far more unsupervised play and childhood independence.”
This is a fairly limited, gentle agenda for school design and other policies, and although I believe Haidt’s talk of “rewiring brains” is mostly ignorable BS, none of his age-limitation rules are incompatible with a free society, and none bear on adults, except in their capacity as teachers and parents.
The “rewiring” talk isn’t BS because it’s necessarily untrue, mind you. Haidt, like Jordan Peterson, is another latter-day Marshall McLuhan — a boundary-defying celebrity intellectual who strategically turns speculation into assertion, and forces us, for better or worse, to re-examine our beliefs. McLuhan preached that new forms of media like movable type or radio do drive neurological change, that they cause genuine warp-speed human evolution — but his attitude, unlike Haidt’s, was that these changes are certain to happen, and that arguing against them was like arguing with the clouds in favour of a sunny day. The children who seem “addicted” to social media are implicitly preparing to live in a world that has social media. They are natives of the future, and we adults are just observers of it.
April 1, 2024
“The loss of capacity for memory or real experience is what makes people susceptible to the work of cartoon pseudo-intellectuals”
Matt Taibbi strongly encourages his readers to exercise their brains, get out of the social media scroll-scroll-scroll trap, and stay sane:

After a self-inflicted wound led to Twitter/X stepping on my personal account, I started to worry over what looked like the removal of multiple lanes from the Information Superhighway. Wikipedia rules tightened. Google search results seemed like the digital equivalent of a magician forcing cards on consumers. In my case, content would often not even reach people who’d registered as social media followers just to receive those alerts.
I was convinced the issue was political. There was clear evidence of damage to the left and right independents from companies like NewsGuard, or the ideologically-driven algorithms behind Google or Amazon ad programs, to deduce the game was rigged to give unearned market advantages to corporate players. The story I couldn’t shake involved video shooter Jon Farina, whose footage was on seemingly every cable channel after J6, but which he himself was barred from monetizing.
Now I think differently. After spending months talking to people in tech, I realize the problem is broader and more unnerving. On top of the political chicanery, sites like Twitter and TikTok don’t want you leaving. They want you scrolling endlessly, so you’ll see ads, ads, and more ads. The scariest speech I heard came from a tech developer describing how TikTok reduced the online experience to a binary mental state: you’re either watching or deciding, Next. That’s it: your brain is just a switch. Forget following links or connecting with other users. Four seconds of cat attacking vet, next, five ticks on Taylor Ferber’s boobs, next, fifteen on the guy who called two Chinese restaurants at once and held the phones up to each other, next, etc.
Generations ago it wasn’t uncommon for educated people to memorize chunks of The Iliad, building up their minds by forcing them to do all the rewarding work associated with real reading: assembling images, keeping track of plot and character structure, juggling themes and challenging ideas even as you carried the story along. Then came mass media. Newspapers shortened attention span, movies arrived and did visual assembly for you, TV mastered mental junk food, MTV replaced story with montages of interesting nonsensical images, then finally the Internet came and made it possible to endlessly follow your own random impulses instead of anyone else’s schedule or plot.
I’m not a believer in “eat your vegetables” media. People who want to reform the press often feel the solution involves convincing people that [they] just should read 6,000-word ProPublica investigations about farm prices instead of visiting porn sites or watching awesome YouTube compilations of crane crashes. It can’t work. The only way is to compete with spirit: make articles interesting or funny enough that audiences will swallow the “important” parts, although even that’s the wrong motive. Rolling Stone taught me that the lad-mag geniuses that company brought in in the nineties, who were convinced Americans wouldn’t read anything longer than 400 words in big type, were wrong. In fact, if you treat people like grownups, they tend to like a challenge, especially if the writer conveys his or her own excitement at discovery. The world is a great and hilarious mystery and if you don’t have confidence you can make the story of it fun, you shouldn’t be in media. But there is one problem.
Inventions like TikTok, which I’m on record saying shouldn’t be banned, are designed to create mentally helpless users, like H addicts. If you stand there scrolling and thinking Next! enough, your head will sooner or later be fully hollowed out. You’ll lose the ability to remember, focus, and decide for yourself. There’s a political benefit in this for leaders, but more importantly there’s a huge commercial boon. The mental jellyfish is more susceptible to advertising (which of course allows firms to charge more) and will show less and less will over time to walk out of the Internet’s various brain-eating chambers.
A cross of Jimmy Page and Akira Kurosawa probably couldn’t invent long-form content to lure away the boobs-and-cat-video addicts these sites are making. The loss of capacity for memory or real experience is what makes people susceptible to the work of cartoon pseudo-intellectuals like Yuval Noah Harari, who seem really to think nothing good or interesting happened until last week. The profound negativity of these WEF-style technocrats about all human experience until now reminds me of Ray Bradbury’s Fahrenheit 451, whose dystopian characters feared books because “They show the pores of the face of life”.
March 14, 2024
“The dark world of pediatric gender ‘medicine’ in Canada”
The release of internal documents from the World Professional Association for Transgender Health (WPATH) revealed just how little science went into many or most juvenile gender transitions and how much the process was being driven politically rather than scientifically. Shannon Douglas Boschy digs into how the WPATH’s methods are implemented in Canada:
An undercover investigation at a Quebec gender clinic recently documented that a fourteen-year-old girl was prescribed testosterone for the purpose of medical gender transition within ten minutes of seeing a doctor. She received no other medical or mental health assessment and no information on side-effects. This is status quo in the dark world of pediatric gender “medicine” in Canada.
On March 5th Michael Shellenberger, one of the journalists who broke the Twitter Files in 2022, along with local Ottawa journalist Mia Hughes, released shocking leaks from inside WPATH, the organization that proclaims itself the global scientific and medical authority on gender affirming care. The World Professional Association of Transgender Health is the same organization that the Quebec gender clinic, and Ottawa’s CHEO, cite as their authority for the provision of sex-change interventions for children.
These leaks expose WPATH as nothing more than a self-appointed activist body overseeing and encouraging experimental and hormonal and surgical sex-change interventions on children and vulnerable adults. Shellenberger and Hughes reveal that members fully understand that children cannot consent to loss of fertility and of sexual function, nor can they understand the lifetime risks that will result from gender-affirming medicalization, and they ignore these breaches of medical ethics.
The report reveals communication from an “Internal messaging forum, as well as a leaked internal panel discussion, demonstrat(ing) that the world-leading transgender healthcare group is neither scientific nor advocating for ethical medical care. These internal communications reveal that WPATH advocates for many arbitrary medical practices, including hormonal and surgical experimentation on minors and vulnerable adults. Its approach to medicine is consumer-driven and pseudoscientific, and its members appear to be engaged in political activism, not science.”
These findings have profound implications for medical and public education policies in Canada and raise serious concerns about the practices of secret affirmations and social transitions of children in local schools.
These leaks follow on the recent publication of a British Medical Journal study (BMJ Mental Health), covering 25-years of data, dispelling the myth that without gender-affirmation that children will kill themselves. The study, comparing over 2,000 patients to a control population, found that after factoring for other mental health issues, there was no convincing evidence that children and youth who are not gender-affirmed were at higher risk of suicide than the general population.
In the last week, a second study was released, this one from the American Urology Association, showing that post-surgical transgender-identified men, who underwent vaginoplasty, have twice the rate of suicide attempts as before affirmation surgery, and showing that trans-identified women who underwent phalloplasty, showed no change in pre-operative rates of suicide and post-operative.
These and other studies are now thoroughly debunking the emotional blackmail myths promoted by WPATH, that the absence of sex-change interventions, suggest that gender-distressed children are at high risk of taking their own lives.
March 11, 2024
“Is it possible that the new therapy culture and the emphasis on introspection is actually making things worse?”
In Quillette, Brandon McMurtrie asks us to consider why, with more people in therapy than ever before, the overall mental health of the population is declining:
Why has mental health got worse given the prevailing emphasis on self-care and accurately knowing and expressing oneself? And why do people and groups most inclined to focus on their identity appear to be the most distressed, confused, and mentally unwell? Is it possible that the new therapy culture and the emphasis on introspection is actually making things worse?
I am not the first to notice these developments — Abigail Shrier’s new book Bad Therapy has carefully delineated a similar argument. Her arguments are elsewhere supported by research on semantic satiation and ironic uncertainty, the effects of mirror gazing, the effects of meditation, and how all this relates to the constant introspection encouraged by therapy culture and concept creep.
Satiation and Its Effects
Semantic satiation is the uncanny sensation that occurs when a word or sentence is repeated again and again, until it appears to become foreign and nonsensical to the speaker. You may have done this as a child, repeating a word in quick succession until it no longer seems to be recognizable. It’s a highly reliable effect — you can try it now. Repeat a word to yourself quickly, out loud, for an extended period, and really focus on the word and its meaning. Under these circumstances, most people experience semantic satiation.
This well-studied phenomenon — sometimes called “inhibition”, “fatigue”, “lapse of meaning”, “adaptation”, or “stimulus satiation” — applies to objects as well as language. Studies have found that compulsive staring at something can result in dissociation and derealization. Likewise, repeatedly visually checking something can make us uncertain of our perception, which results, paradoxically, in uncertainty and poor memory of the object. This may also occur with facial recognition.
Interestingly, a similar phenomenon can occur in the realm of self-perception. Mirror gazing (staring into one’s own eyes in the mirror) may induce feelings of depersonalization and derealization, causing distortions of self-perception and bodily sensation. This persistent self-inspection can result in a person feeling that they don’t recognize their own face, that they no longer feel real, that their body no longer feels the same as it once did, or that it is not their body at all. Mirror-gazing so reliably produces depersonalization and realization (and a wide range of other anomalous effects), that it can be used in experimental manipulations to trigger these symptoms for research purposes.
[…]
The Satiation of Gender Identity
The number of people identifying as non-binary or trans has skyrocketed in recent years, and a growing number of schools are now teaching gender theory and discussing it with children — sometimes in kindergarten, more often in primary school, but especially in middle- and high-school (though in other schools it is entirely banned). While this may be beneficial for those already struggling with gender confusion, it may also present an avenue for other children to ruminate and become confused via “identity satiation”.
The kind of gender theory increasingly taught in schools encourages children to spend extended periods of time ruminating on self-concepts that most would not otherwise have struggled with. They are given exercises that encourage them to doubt their own unconscious intuitions about themselves, and to ruminate on questions like “Do I feel like a boy?” and “What does it mean to feel like a boy?” and “I thought I was a boy but what if I am not?”
Such questions are often confusing to answer and difficult to express, even for adults unaffected by gender dysphoria. But asking children to ruminate in this way may lead to confusion and depersonalization-derealization via the mechanisms described above. “Identity satiation” may then lead them to decide they are non-binary or trans, especially when identifying as such is rewarded with social recognition and social support. Many people who subsequently de-transitioned have described this process: “I never thought about my gender or had a problem with being a girl before”.
March 10, 2024
The rapid transition from the amazing smartphone to the “pocket moloch”
Magdalene J. Taylor follows up her New York Times article from last year with more evidence that so many of the social problems identified today are caused by, or at least made worse, by the almost universal addiction to smartphones:
A year ago, I published an opinion essay for the New York Times that changed the trajectory of my career. It was about how fewer Americans are having sex, across nearly every demographic. For any of the usual caveats — wealth, age, orientation — the data almost always highlighted that previous generations in the same circumstances were having more sex than we are today. My purpose in writing the essay was mainly to try to emphasize the role that sex plays in our cultural wellbeing its connection to the loneliness epidemic. Many of us have developed a blasé attitude toward sex, and I wanted people to care. It wasn’t really about intercourse, and I said as much. It was about wanting to live in an lively, energetic society.
Since writing, I have been continuously asked what I think the cause of all this is. Obviously, there isn’t one universal answer. After publishing, I went on radio shows and podcasts and was asked to share what I thought some of them could be. Economic despair, political unrest, even climate fears were among the reasons I’d heard cited. But all of that, honestly, feels pointlessly abstract. It puts the problem entirely out of our hands, when in fact I believe it may quite literally be in them.
The problem is obviously our phones.
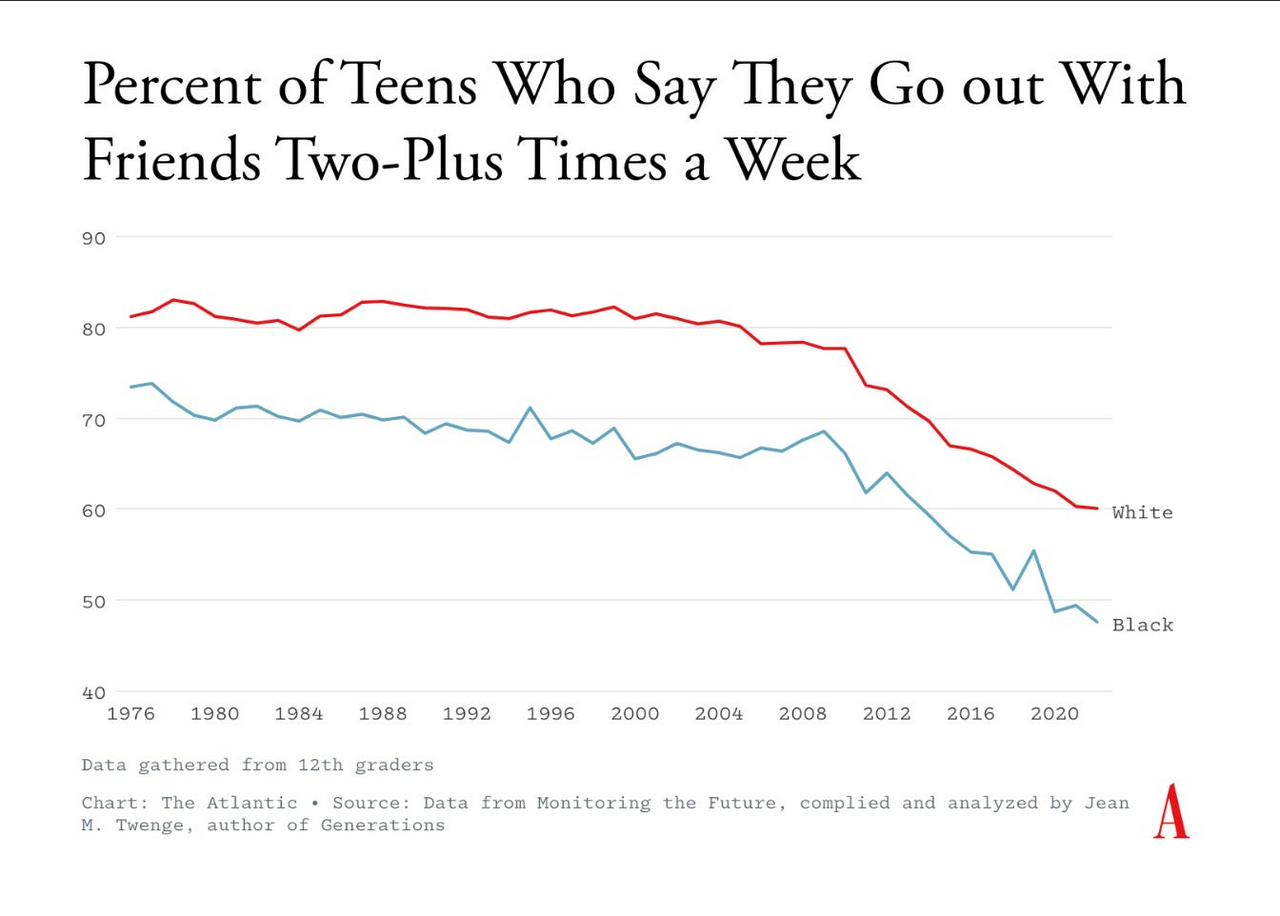
In February, The Atlantic published a feature about the decline of hanging out. Within it was a particularly damning graph sharing the percentage of teens who report hanging out with friends two or more times per week since 1976. Rates were steady around 80 percent up until the mid-90s, when a subtle decrease began to occur. Then, in 2008 — one year after the release of the first iPhone — the decrease became much more dramatic. It has continued falling sharply since, hovering now at just under 60 percent of teens who spend ample time with friends each week.
Some of us really don’t like our screen time habits criticized. Others may think they appear smarter by highlighting other issues, that they can see above the fray and observe the macro trends that are really shaping our lives, not that stupid anti-phone rhetoric we hear from the Boomers. And some of these other trends do indeed apply. Correlation does not equal causation. Lots of things happened in 2008. Namely, a financial crisis the effects of which many argue we are still experiencing. When I shared the graph on Twitter/X saying phones are the obvious cause, this was one of the most common rebuttals. Another was the decline in third spaces. There are indeed few places for teenagers to hang out outside of the home. Skate parks are being turned into pickleball courts with “no loitering” signs, malls are shuttering and you can no longer spend $1 on a McChicken to justify hanging out in the McDonald’s dining area for hours. But as the Atlantic piece explains, the dwindling of places to be and experience community has a problem we’ve been lamenting since the 90s. And it’s not just teens — everyone is spending less time together than they used to. “In short, there is no statistical record of any other period in U.S. history when people have spent more time on their own,” the article states.
March 6, 2024
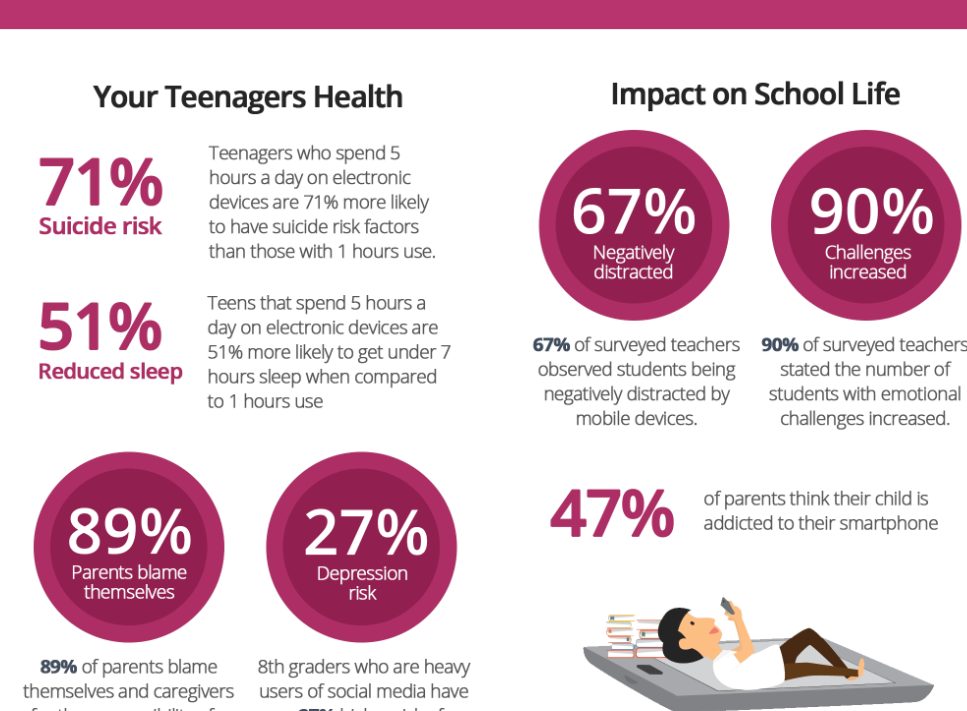
Ted Gioia on escaping from the trap of Dopamine Culture
Following up on this hot issue, Ted Gioia has some suggestions to get out of the habit:
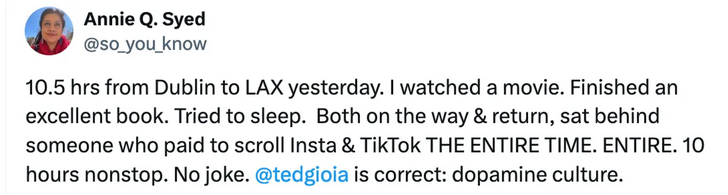
My dopamine culture essay is still stirring up lots of discussion. And people have their own stories to share.
For example:
And also:
The same thing is happening everywhere — at concerts, at museums, at work, at church, while driving, or even at a funeral.
But it’s even worse when people don’t even try to multitask, instead abandoning essential life tasks—because of the compulsion to scroll.
I’ve now heard from
- People who scroll instead of sleeping
- People who scroll instead of engaging in physical activity
- People who scroll instead of finding a life partner, or connecting with flesh-and-blood people
- People who scroll instead of gaining skills, finding a job, and pursuing a vocation
- Etc.
I originally focused on the impact on arts and creativity—because that’s the world I live in. I was worried that people had no patience for a movie or concert or book, because they can only digest stimuli in 15-second bursts.
But I now see that the problem is much, much bigger.
It’s almost quaint to worry about these screen zombies not reading books. The simple fact is that, increasingly, their entire life is suffering because of a technology shift imposed on them by Silicon Valley.
These addictive and compulsive behaviors are troubling. But even more disturbing is how the largest corporations in the world are investing billions in promoting and accelerating this compulsive use of their tech tools.
If you look at the 10 largest companies in the world, half of them are trying to create this addictive relationship to technology. The days when the dealer in addiction had to hide in the shadows are over. They now operate freely in your home, and every other sphere of your life.
A few days ago, I promised to offer concrete suggestions for dealing with this. Some of these are listed below.
February 26, 2024
Time to pry the smartphones from the clutches of our dopamine-addicted youngsters?
A couple of articles this weekend deal with the already acknowledged problem of dopamine addiction especially among the young whose brains and personalities are still in the formative stages. First, here’s Christopher Gage reporting with some delight that British schoolchildren are going to have to learn how to cope with a full school day without the electronic binkies they’ve grown so dependent on:
Detail of an article at bankmycell.com
I long for the day when gawking at one’s phone like a lobotomy patient invokes derision. Don’t you know your filthy addiction pollutes every atom of our society? You selfish bastard. You perverts should be ashamed of yourselves, etc. That day is on the horizon.
This week, British lawmakers banned smartphones in schools. Those pocket perils are lobotomising those whom sentimentalists call “the nation’s future”. Denied their devil devices, schoolchildren will endure hours of reading, thinking, and writing. Heaven forbid, they’ll talk to their friends and teachers in flesh and blood.
In these matters, I am militant. Children are not vessels of wisdom and wonder corrupted by a cruel world. They’re ignorant. By teaching them how to think and live, adults civilise children. That bleeping burping buzzing beehive in their pockets renders that civilising mission impossible.
Many disagree. But their knee-jerk reaction to this “knee-jerk reaction” crashes against concrete evidence. Smartphones erode concentration, dull critical thinking, blunt memory, and shred retention. The monstrous equation: Smartphones plus face-hugger apps equals ignorant, depressed, anxious youths.
Yes, technology invites moral panic. Plato worried that the written word would mulch minds into mush. But this is serious.
Last year, Dr Vivek Murthy, the United States surgeon general, issued a rare public health advisory. Across 19 pages, Dr Murthy warned that the effects of social media on adolescent mental health were “not fully understood”.
“There are ample indicators that social media can also have a profound risk of harm to the mental health and well-being of children and adolescents,” he said.
And what did we say? Not much. We had more important matters to attend. If I remember correctly, on that very day, Kim Kardashian revealed on Instagram her latest arse or her newest boyfriend.
However, serious people think this is a serious problem. Dr Benjamin Maxwell, a director of child and adolescent psychiatry at Rady Children’s Hospital in San Diego, said he is “immensely concerned” by a study linking social media and poor mental health. That “highly stimulating environment” may corrode “cognitive ability, attention span and memory during a time when their brains are still developing,” Maxwell said. “What are the long-term consequences? I don’t think we know.”
The UN’s education, science, and culture agency says the more young Jack scrolls through TikTok and the like, the lower his grades sink.
Countless studies show smartphones and their face-hugger apps — designed by behavioural psychologists to addict and milk the user — worsen anxiety, depression, and self-esteem. Not to mention lining up children for the predation of bullies 24/7.
Psychologists Jonathan Haidt and Jean Twenge are the canaries in the cultural coalmine. They say HMS Progress is crashing toward the icebergs — rising rates of suicide, depression, and anxiety. To them, the evidence is almost irrefutable. Turn back now, they say, or the ship sinks.
The second item is a follow-up by Ted Gioia to his post on dopamine culture last week:
My article on “dopamine culture” has stirred up interest and (even more) raised concerns among readers who recognize the symptoms I described.
One of the illustration went viral in a big way. And I’ve gotten requests from all over the world for permission to translate and share the material. (Yes, you can all quote generously from the article, and reprint my charts with attribution.)
This image was shared widely online
But many have asked for more specific guidance.
What can we do in a culture dominated by huge corporations that want us to spend hours every day swiping and scrolling?
I find it revealing and disturbing that readers who work on the front lines (in education, therapy, or tech itself) expressed the highest degree of alarm. They know better than anybody where we’re heading, and want to find an escape path.
Here’s a typical comment from teacher Adam Whybray:
I see it massively as a teacher. Kids desperately pleading for toilet breaks, claiming their human rights are being infringed, so they can check TikTok, treating lessons as though they’re in a Youtube reaction video, needing to react with a meme or a take — saying that silence in lessons scares them or freaks them out.
One notable difference from when I was at school was that I remember a lesson in which we got to watch a film was a relief or even pleasurable (depending on the film). My students today often say they are unable to watch films because they can’t focus. I had one boy getting quite emotional, begging to be allowed to look at his phone instead.
Another teacher asked if the proper response is to unplug regularly? Others have already embraced digital detox techniques of various sorts (see here and here).
I hope to write more about this in the future.
In particular, I want to focus on the many positive ways people create a healthy, integrated life that minimizes scrolling and swiping and mindless digital distractions. Many of you have found joy and solace — and an escape from app dependence — in artmaking or nature walks or other real world activities. There are countless ways of being-in-the-world with contentment and mindfulness.
Today I want to discuss just one bedrock of real world life that is often neglected — or frequently even mocked: Ritual.
I know how much I rely on my daily rituals as a way of creating wholeness and balance. I spend every morning in an elaborate ritual involving breakfast, reading books (physical copies, not on a screen), listening to music, and enjoying home life.
Even my morning coffee preparation is ritualistic. (However, I’m not as extreme as this person — who rivals the Japanese tea ceremony in attention to detail.)
I try to avoid plugging into the digital world until after noon.
I look forward to this daily time away from screens. But my personal rituals are just one tiny example. There are many larger ways that rituals provide an antidote to the more toxic aspects of tech-dominated society.
Below I share 13 observations on ritual.
February 16, 2024
“… the rise in emotional disturbance among young women correlates precisely with the introduction of the smart phone”
At Postcards from Barsoom, John Carter sets off all the alarms with a proposal to address the burgeoning issue of social media addiction and the closely correlated rise in mental health issues among young women:

The psychic breakdown of the young Western female has been the defining political phenomenon of the twenty-first century. Women are suffering from depression, anxiety, neurosis, and dysphoria as never before, they’re drugged to the gills to deal with it, and they’ve got the SSREyes to prove it.
This isn’t only a problem for young women. Their suffering is everyone’s suffering. The romantic paranoia engendered by MeToo, a mass hysteria that has grown directly out of this plague of neurosis, has destroyed courtship among the young. As a result a shocking fraction of young men are virgin incels, while their femcel counterparts are contemplating a future where 45% of them will be childless. Driven by their neglected ovaries to latch on to surrogate children in the form of migrants and minorities, and entering into lesbian civil unions with the Mammy State, childless women overwhelmingly vote left – as always, the party of the psychically distressed thrives to whatever degree it cultivates psychic distress. The political derangement is downstream of their emotional derangement, and the two feed on one another in a vicious spiral of crazed minds pushing crazed policies that craze minds yet further, a cycle that threatens to break civilization, either gradually through steady demographic deflation and spiritual demoralization, or perhaps – if the young men alienated by a society that has ruined their women cease stupefying themselves with porn, and cohere as an army – more catastrophically.
There’s no real mystery as to why this has happened.
Jonathan Haidt has demonstrated at length and in extraordinary empirical detail that the rise in emotional disturbance among young women correlates precisely with the introduction of the smart phone, and the mass migration of social lives onto social media that immediately followed. The slot machine engineers of Silicon Valley trapped the world’s young women in a Skinner box by hacking their instinctive sexual competition strategies. Suddenly every young girl in the world was measuring herself against every other young woman, all viewing one another through the distorting filters of flattering camera angles, ruthlessly curated digital photographs, makeup, plastic surgery, and AI filters that smoothed wrinkles, removed blemishes, and reduced unwelcome poundage. On the Internet no girl is ever the prettiest girl in the room, or even the second or third prettiest. Meanwhile they’re flooded with a relentless barrage of that most intoxicating of drugs: male attention.
Of course they went mad.
They’re all wandering around in a state of selfie-shock.


