
At Mother Jones, Kevin Drum links to an article that explicitly shows the cost of having monopoly providers in healthcare:
Regular readers of this blog should know that when it comes to the price of hospital care, it’s competition that matters, not insurance companies. In areas with only a single hospital, insurance companies have no leverage and have to accept whatever price the hospital charges. If there are lots of hospitals, they have to compete with each other to earn the insurance company’s business.
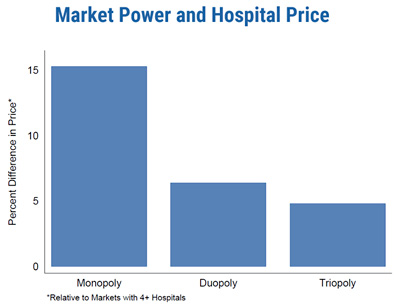
But in case you’re still skeptical, a team of researchers has analyzed a huge database of health care claims in the US to check this out. They found enormous regional variation in hospital costs for the same procedure, and one of the biggest drivers of this variation was competition:
Hospital market structure stands out as one of the most important factors associated with higher prices, even after controlling for costs and clinical quality. We find that hospitals located in monopoly markets have prices that are about 15.3 percent higher than hospitals located in markets with four or more providers. This result is robust across multiple measures of market structure and is consistent in states where the HCCI data contributors (and/or Blue Cross Blue Shield insurers) have high and low coverage rates.
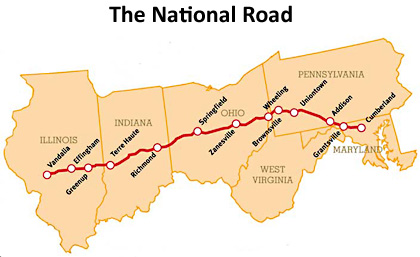 Professional painters in the 1800s prepared house paint by mixing linseed oil with white lead paste. About 90% of Americans lived in rural areas in the mid-1800s, and subsistence farmers could make linseed (flaxseed) oil, but few had access to white lead, so they mixed linseed oil with red rust to kill fungi that trapped moisture and increased wood decay. Red barns are still a tradition in most USA farming regions but white barns are the norm along the path of the old National Road. Why?
Professional painters in the 1800s prepared house paint by mixing linseed oil with white lead paste. About 90% of Americans lived in rural areas in the mid-1800s, and subsistence farmers could make linseed (flaxseed) oil, but few had access to white lead, so they mixed linseed oil with red rust to kill fungi that trapped moisture and increased wood decay. Red barns are still a tradition in most USA farming regions but white barns are the norm along the path of the old National Road. Why?

