
Eric Boehm tries to sort out where the startling claim came from … because it’s not true:
While reading about the COVID-19 outbreak, you’ve probably encountered this particularly shocking statistic at one time or another: 80 percent of America’s pharmaceutical drug supply comes from China.
It’s a statistic that has made the rounds in right-wing publications for a while — offered as proof that China-heavy global supply chains are putting Americans at risk — but it has also popped up in mainstream outlets, including in pieces published in Politico and The Atlantic. Wherever it is deployed, the stat carries an unstated implication: What if China decides to cut us off in the middle of a pandemic? Could America face a dramatic shortage of key pharmaceutical drugs at the moment when we are most in need? And that distorted claim that says America has been too reliant on China has been seized by politicians like Sen. Josh Hawley (R–Mo.) as evidence that globalization has undermined America’s pandemic response.
[…]
How much is a lot? “In all, 80 percent of the U.S. supply of antibiotics are made in China,” [Politico contributors Doug Palmer and Finbarr Bermingham] wrote, linking back to a press release from Sen. Chuck Grassley (R–Iowa).
But that’s not what the press release says.
Grassley’s statement was publicizing a letter Grassley sent on August 9 to the Department of Health and Human Services (HHS) and the FDA, asking them to conduct more inspections of foreign drug manufacturing facilities to make sure they meet American standards.
“Unbeknownst to many consumers … 80 percent of Active Pharmaceutical Ingredients are produced abroad, the majority in China and India,” Grassley wrote.
There’s the first bit of context collapse: the authors of the Politico piece merged Grassley’s “80 percent … are produced abroad” into “80 percent … are made in China.”
All of this also raises another question: Where is Grassley getting that information? His letter sources that claim to a 2016 Government Accountability Office report which itself cited FDA data on pharmaceutical manufacturers around the world. And that report makes it clear that the U.S. has a diverse supply chain for drugs that goes well beyond India and China.
“Nearly 40 percent of finished drugs and approximately 80 percent of active pharmaceutical ingredients (API) are manufactured in registered establishments in more than 150 countries,” is how the GAO summed up America’s pharmaceutical supply chain.
In two jumps, we’ve gone from “80 percent of American drugs are manufactured in more than 150 countries around the world” to “80 percent of drugs come from two countries” to “80 percent of drugs come from China.”
Now, a further complication. The FDA only tracks drug manufacturing facilities — not the supply chains of specific drugs.
That “lack of structural transparency and available supply chain data about drugs,” researchers at the University of Minnesota researchers wrote last month, is one of the reasons why making accurate assessments about potential drug shortages is difficult. Indeed, it was this same bit of missing information that Grassley was encouraging the FDA to address back in August.
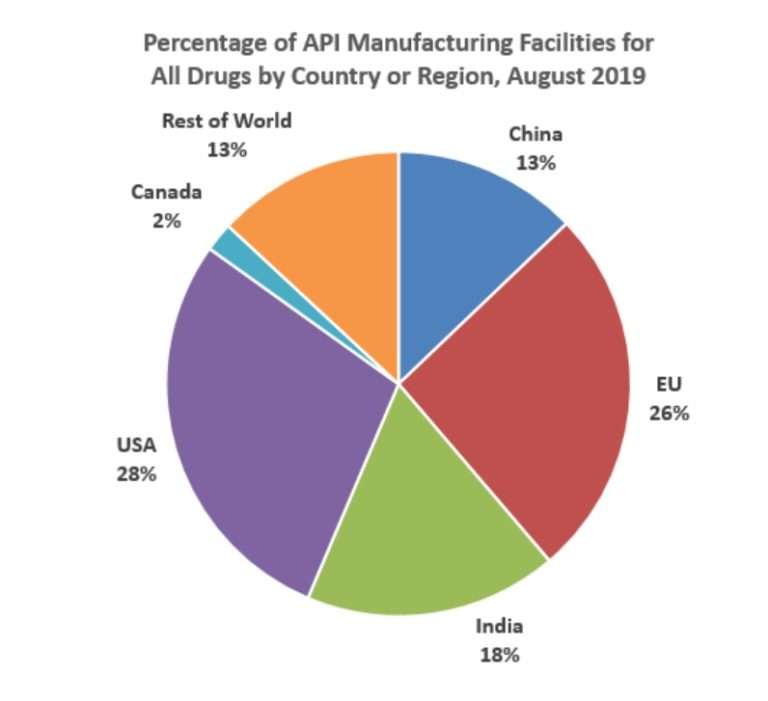
Source: FDA; Safeguarding Pharmaceutical Supply Chains in a Global Economy, October 2019.




