
… these same people want the government to provide them with free health care, and if they got their full way, other “positive liberties” (to quote Obama) including free college, free housing, free food, guaranteed income, guaranteed jobs.
[…] the moment all your necessities are furnished by someone else, someone else gets to make all the decisions for you. I mean, if your health is paid for by the taxes of your fellow citizens, and the government aka the nation looks after your every need: should they pay for your health if you insist on smoking or drinking? Or should those resources be husbanded for people who take better care of themselves? Okay, Sarah, but isn’t there a point to individual responsibility? Why shouldn’t you be required to take minimal care of yourself, so you get the benefits of the government’s care, which as you say someone else pays for.
Ah, but there’s the rub. See, ultimately, there’s always something some of us say or do that can be used to justify denying care or giving only palliative care. For instance, I’m overweight, which seems to be one of the remaining sins in the current lexicon. Sure, I gained tons of weight over 20 years of untreated hypothyroidism, even though I was starving myself for a long portion of those. But hey, I allowed myself to be overweight. So my prognosis is poor. Why spend money on me, when someone else could have better results?
Hell, even when it comes to my autoimmune. I’m a poor prospect, so why give me top of the line care?
If the government controlled other things, it would be exactly the same. Food? Sure, I break out in eczema all over when I eat a diet rich in carbs. But hey, flour and rice are cheap, and why should I get a specialized diet, since I’m only a writer who isn’t even a leftist or a supporter of the state, and besides my prospects of survival are poor?
College? Sure you want to be an economist, but your teachers say you’re cheeky and talk back, and the state doesn’t need that. What we need right now are pipe fitters. Here, you can take this six week course.
When the state is paying the bill, the state gets to decide what is better for you. The European constitution gives you the right to “death with dignity” because death with dignity is much cheaper than expensive treatments with a low chance of survival. After all this money is for everyone, you know?
And like the NHS, in Britain, they won’t even let you seek treatment outside their tender mercies. Why should they? They pay for you. That means in the end they decide what to spend on you. They own you. And if you went outside their system and your kid got cured? It would look pretty bad for them, wouldn’t it? Why should they allow you to do that? And besides, peasant, you have a bad attitude.
Sarah Hoyt, “Slouching Into Shackles”, According to Hoyt, 2018-04-27.
July 25, 2020
July 6, 2020
The Healthcare Crisis of 1941 – WW2 – On the Homefront 005
World War Two
Published 2 Jul 2020When WWII breaks out many parts of the world are still missing population-wide healthcare. The pressure of the war deteriorates healthcare services even further. By 1941, both the British Commonwealth and Germany are facing an outright healthcare crisis on the home front.
Join us on Patreon: https://www.patreon.com/TimeGhostHistory
Or join The TimeGhost Army directly at: https://timeghost.tvFollow WW2 day by day on Instagram @World_war_two_realtime https://www.instagram.com/world_war_two_realtime
Between 2 Wars: https://www.youtube.com/playlist?list…
Source list: http://bit.ly/WW2sourcesHosted by: Anna Deinhard
Written by: Fiona Rachel Fischer and Spartacus Olsson
Director: Astrid Deinhard
Producers: Astrid Deinhard and Spartacus Olsson
Executive Producers: Astrid Deinhard, Indy Neidell, Spartacus Olsson, Bodo Rittenauer
Creative Producer: Joram Appel
Post-Production Director: Wieke Kapteijns
Research by: Fiona Rachel Fischer
Edited by: Mikołaj Cackowski
Sound design: Marek Kamiński
Map animations: Eastory (https://www.youtube.com/c/eastory)Sources:
IWM D 2373, D 2318, B 14299, D 2315, D 2078, D 14318, D 2334
Narodowe Archiwum Cyfrowe
Bundesarchiv
Wellcome Images no. L0028759
From the Noun Project: london by Pablo Fernández Vallejo, Patient by Miho Suzuki-Robinson, Patient by Binpodo, Doctor by Wilson Joseph, Hospital by Hare Krishna, School by David, Apartment by Victoruler, Bus by Eucalyp
University of Liverpool Faculty of Health & Life SciencesSoundtracks from the Epidemic Sound:
Farrell Wooten – “Blunt Object”
Johannes Bornlof – “Deviation In Time”
Skrya – “First Responders”
Gunnar Johnsen – “Not Safe Yet”
Johannes Bornlof – “The Inspector 4”
Jon Bjork – “For the Many”
Reynard Seidel – “Deflection”
Rannar Sillard – “March Of The Brave 4”
Cobby Costa – “From the Past”
Fabien Tell – “Last Point of Safe Return”
Cobby Costa – “Flight Path”
Andreas Jamsheree – “Guilty Shadows 4”
Jo Wandrini – “Puzzle of Complexity”Archive by Screenocean/Reuters https://www.screenocean.com.
A TimeGhost chronological documentary produced by OnLion Entertainment GmbH.
From the comments:
World War Two
2 days ago (edited)
It might be surprising that the global healthcare crisis of 2020 has an immediate relationship to WW2, but it does. Although, when you look at it, it’s logical — with every crisis humanity learns a little — it was still a little bit of a surprise to us how direct this relationship was when researching and writing this episode. Was it surprising to you too?On the topic of writing, this is the first episode by our new co-writer, Fiona Rachel Fischer, who will now be a regular contributor to the On the Homefront series — please give her a warm welcome.

July 3, 2020
Back to the Future Middle Ages
At Spiked, Dominic Frisby takes us back to a time when today’s progressive temper tantrums would fit in perfectly with accepted behaviours of the age … the Middle Ages:

A social media heretic faces trial
How much of what went on in the Middle Ages and early-modern periods do we look back on with abhorrence and a certain amount of perplexity? Burning witches at the stake, lynch mobs, self-flagellation – what possessed people to do such things, we wonder.
But take a step back, look about and you see many of these practices are still flourishing today, though they go by different names.
Here are just some of them.
Let’s start with excommunication. Excommunication meant so much more than being banned from taking communion. It involved you being shunned, shamed, spiritually condemned, even banished. Only through some kind of heavy penance – often a very public, lengthy and humiliating contrition – could you and your reputation be redeemed.
Excommunication became a powerful political weapon. It was dished out to enemies of the faith to destroy their legitimacy. Often it was used as a punishment for sins as minor as uttering the wrong opinion.
What are No Platforming and cancel culture if not a modern form of excommunication? Qualified, competent professionals are hounded out of their jobs and publicly shamed just for uttering the wrong opinion, often simply for a misjudged choice of words. Even just the wrong pronouns.
As often as not, their employer wants a quiet life, so he bows to activist pressure and sacks the target of the witch hunt. Cancel culture is excommunication.
Today’s religions, however, are not the many sects of Christianity that once perforated Europe, but climate change, education, the NHS, gay rights, trans rights, the European Union and multiculturalism. Even coronavirus and the lockdown have become sacrosanct.
Intellectuals of the right and left, from Polly Toynbee to Nigel Lawson, have described the NHS as Britain’s religion. It has replaced the Virgin Mary as the divine matriarch. Why this worship? I suggest it goes back to the late 19th and early 20th centuries, when the state began to replace the church as the main provider of education, welfare and healthcare. After 1945, it was just a matter of time before the welfare state achieved altar status.
June 14, 2020
Healthcare is a provincial responsibility … thank goodness
Chris Selley reminds us that despite all the attention the media pays to every twitch of the federal government, it’s the provinces that are actually responsible for the healthcare systems in their territory:

Front view of Toronto General Hospital.
Photo via Wikimedia Commons.
Here in Canada, however, astonishing scenes continue. On Thursday the Toronto Transit Commission announced it intends to make masks mandatory for riders — no word of a lie — in three weeks, on July 2. That’s assuming the commission approves the measure … next Wednesday. TTC CEO Rick Leary was at pains to stress the rule would never be enforced.
Meanwhile Theresa Tam, Canada’s chief public health officer, could not appear more reluctant to endorse mask wearing unless she advised against wearing them altogether — which was, famously, her original position. On Wednesday, she unveiled a four-bullet-point plan for getting safely back to semi-normal under the moniker “out smart.” The word “masks” does not appear. Supplementary text only concedes they “can be used … when you can’t maintain physical distance of two metres.”
This is a strange qualification: The official federal advice stresses you shouldn’t touch your mask except to take it off at home and immediately wash your hands. You shouldn’t be taking it on and off while you’re out and about, when social distancing suddenly becomes impossible. But it’s not as strange as the qualification Tam offered on her Twitter account, where she offered a link to an instructional video but only “if it is safe for you to wear a non-medical mask or face covering (not everyone can).”
It is true that some people with asthma or severe allergies have trouble wearing masks. Presumably they know who they are, and would not risk suffocating themselves when mask-wearing isn’t even strongly recommended, let alone mandatory. Blind people will struggle to keep two metres’ distance from others. People with aquagenic urticaria can’t wash their hands with water. People without arms can’t cough into their sleeves. Those “out smart” recommendations aren’t qualified, because that would be silly — as is the qualification on masks.
I would be lying if I said I had any idea what the hell is going on. But this never-ending weirdness is doing us a favour, in a way. The fact is, we have been paying far too much attention to the feds throughout this ordeal. Canada’s COVID-19 experience was always much too different from region to region to justify everyone taking their cues from a single public health agency — let alone one that comprehensively botched something as simple as issuing self-isolation advice to returning foreign travellers.
Canada is a federation by design, not by accident, and thank goodness for that: Far better that most provinces’ authorities did a good job knocking down COVID-19 than that a single one screwed it up for the whole country. It’s something Liberals and New Democrats should bear in mind next time they find themselves demanding yet another “national strategy” in a provincial jurisdiction.
February 19, 2020
Enoch Powell
Theodore Dalrymple reviews a recent book by Paul Corthorn on Powell’s career and the concerns that animated him:
Enoch Powell in a 1987 portrait by Allan Warren.
Wikimedia Commons.
It does not pretend to be a biography, or even an intellectual biography. Rather, it chronicles, scrupulously but somewhat drily, Powell’s varying attitudes toward the main subjects of his political concerns: international relations, economics, immigration, Britain’s relations with Europe, and the status of Northern Ireland in the United Kingdom. Powell’s wider intellectual interests and religious views are scarcely touched upon, though it is mentioned that he went from being a believer to being (under the influence of Nietzsche) an atheist, to then returning to Christian belief. There is no description of his character in this book, not even by implication, and with this book as a guide, one would not recognise him if one met him. It is not possible to tell whether the author admires or detests his subject. This neutrality creates confidence in the accuracy of his scholarship, but also makes his book less than a pleasurable or exciting read. Perhaps it is the sign of a frivolous mind, but I prefer even histories of ideas to be spiced with a little biography (or, more truthfully, gossip).
The author does, however, offer a unifying interpretation of Powell’s various political concerns, namely that they were all responses to Britain’s precipitous national decline, the steepest part of which occurred in his lifetime, but which is continuing apace to the extent that Britain might even cease to be a nation at all. Powell was born in a great power and died in an enfeebled country with no industrial or military might, with precious little patriotism, and with no sense either of grandeur or collective purpose.
That this decline – relative rather than absolute, except in such fields as the maintenance of law and order — was inevitable given the conjunctures of the age, was evident to Powell (though not at first). This relative decline was already implicit in Disraeli’s dictum that “the Continent [of Europe] will not suffer England to be the workshop of the world.”
Powell’s concerns, then, were how to manage Britain’s decline and how to find it a new place in the world. He had not always been perceptive about the scale of its decline. He clung, for example, to the illusion that the Empire might still count for something even after the Second World War. Thereafter, however, he became a devotee of a kind of Realpolitik, to the extent of wanting a rapprochement or even alliance with the Soviet Union to balance the power of the United States, whose aims he had long distrusted. He discounted ideology, including communism, as a force in international politics, which is odd in a man who was by far the most intellectual and intellectually accomplished of all British politicians of the 20th century, being both a classical scholar and a brilliant linguist. He seemed to think that Soviet ambition was merely that of any large power in the great game. Those countries that fell into its grip knew otherwise.
On economics, Powell was an early devotee of the superiority of the market over state planning at a time when the intellectual tide was running the other way. There was one important subject, however, on which he was a confirmed statist, namely that of health care. He was for a time Minister of Health in the British government, during which he fiercely defended the NHS. He believed that the government had an ethical duty to provide health care for its citizenry, and it never seemed to occur to him that the centralised NHS was not the only possible way of doing so. He was often highly suspicious of international comparison, but it is difficult to see how judgment of the merits of a system could be made without it. It was clear, moreover, that in this, as in other fields, Britain was at best very mediocre. Perhaps Powell was blind to the NHS’s mediocre performance because of the benevolence of its stated intentions (an occupational hazard among intellectuals, even — or perhaps especially — among brilliant ones). At any rate, he never satisfactorily explained why health care should be different from other spheres of service provision in the superiority of private over public organization.
March 23, 2019
The NHS, Britain’s “national treasure”, gets panned by other EU patients who’ve experienced non-NHS care
In The Conversation, Chris Moreh, Athina Vlachantoni, and Derek McGhee report that — contrary to British myth-making — the National Health Service isn’t the envy of the civilized world:
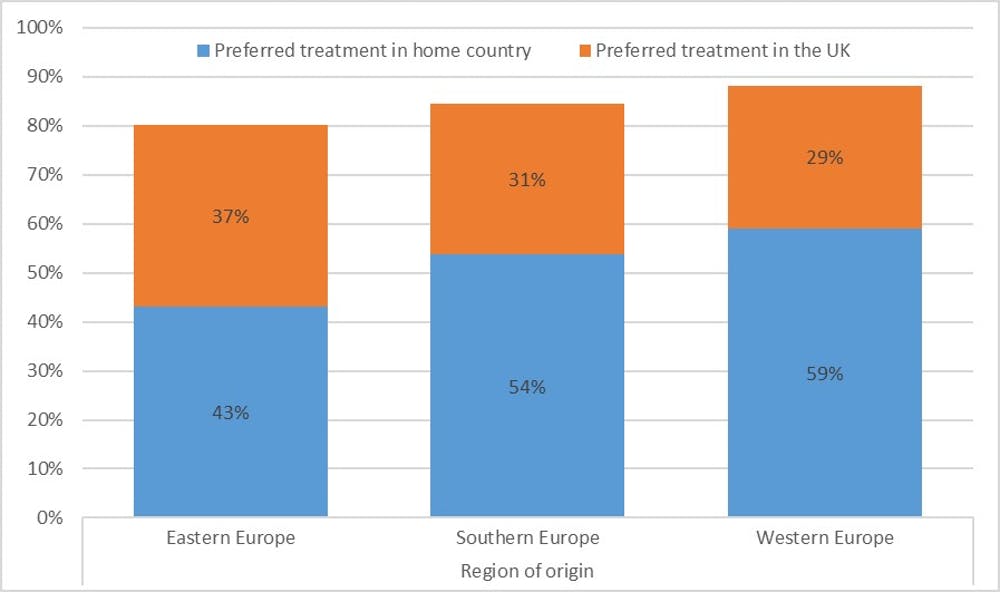
Britain’s National Health Service is often described as a “national treasure”. And it is a sentiment those on the left and the right of the political divide agree on. The British public are so proud of the NHS, they made it the central theme of the opening ceremony of the 2012 London Olympic Games.
But this pride has also been coupled with fears that the universal healthcare provided by the NHS might be taken advantage of by patients from outside the UK. A few months after the Olympics, the then health secretary, Jeremy Hunt, felt the need to clarify that “we are a national health service, not an international health service”. The 2015 election-winning manifesto of the Conservative party made this point even clearer when it pledged to “tackle health tourism” and “recover up to £500m from migrants who use the NHS”.
But our research shows that while the NHS may be a national treasure to British people, EU migrants would rather be treated in their countries of origin. As a 38-year-old woman from Germany put it: “Sorry, NHS? No thanks.” And the reasons for rejecting the NHS? A 25-year-old man from the Netherlands says it’s because the “NHS is slow and the medical care mediocre”. Or, at least, it “is rather poor compared to healthcare in my country,” says a 45-year-old woman from Germany.
But why should British people worry about what EU migrants think of their health service? What EU migrants think and choose is important because they are familiar with at least two European healthcare systems. They have the information and personal experience that most British citizens do not. There is a lot to be learnt from them.


